

Personalized RNA neoantigen vaccines stimulate T cells in pancreatic cancer
- PMID: 37165196
- PMCID: PMC10171177
- DOI: 10.1038/s41586-023-06063-y
Personalized RNA neoantigen vaccines stimulate T cells in pancreatic cancer
Abstract
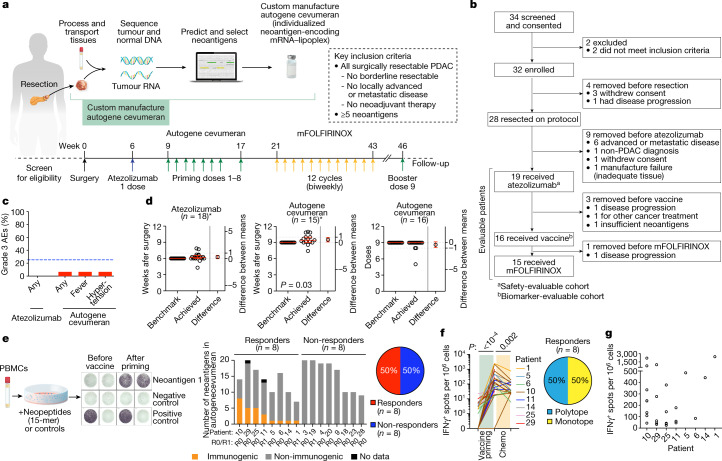
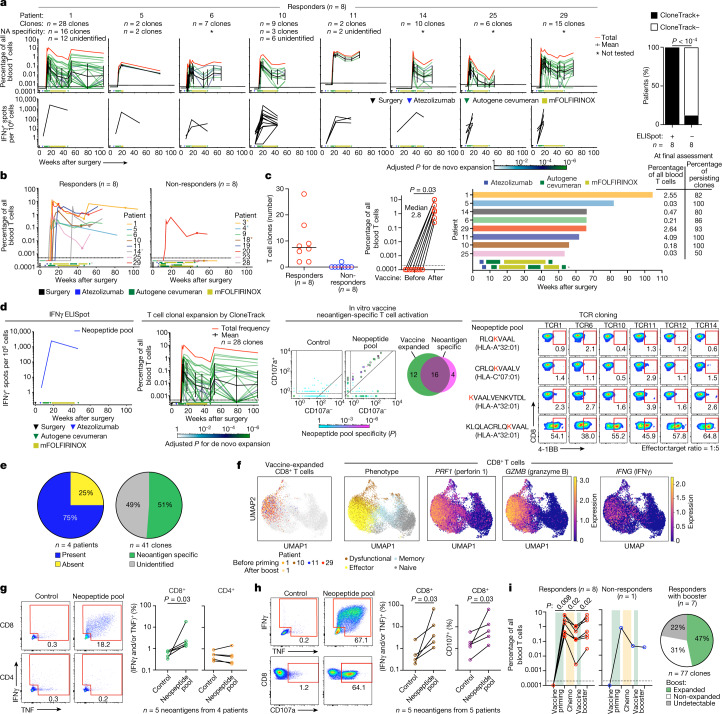
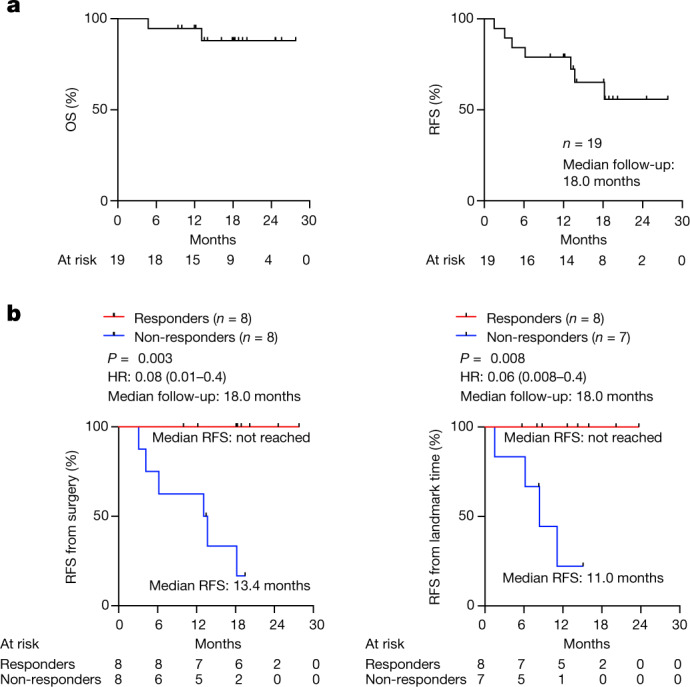
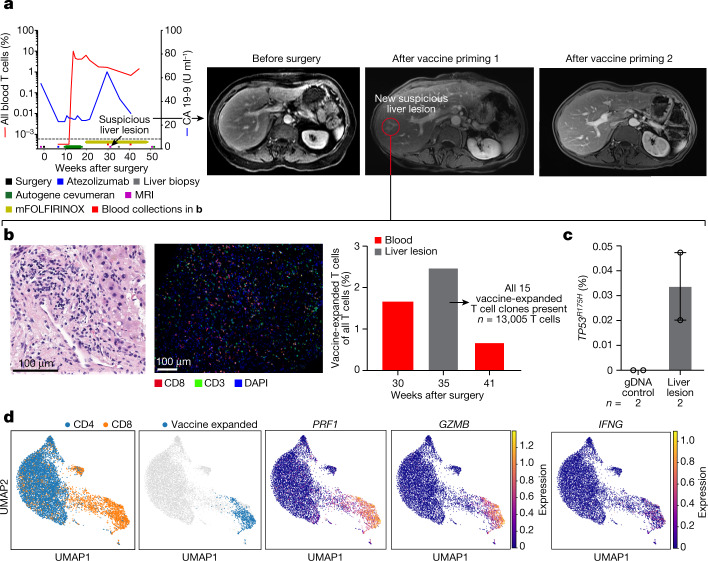
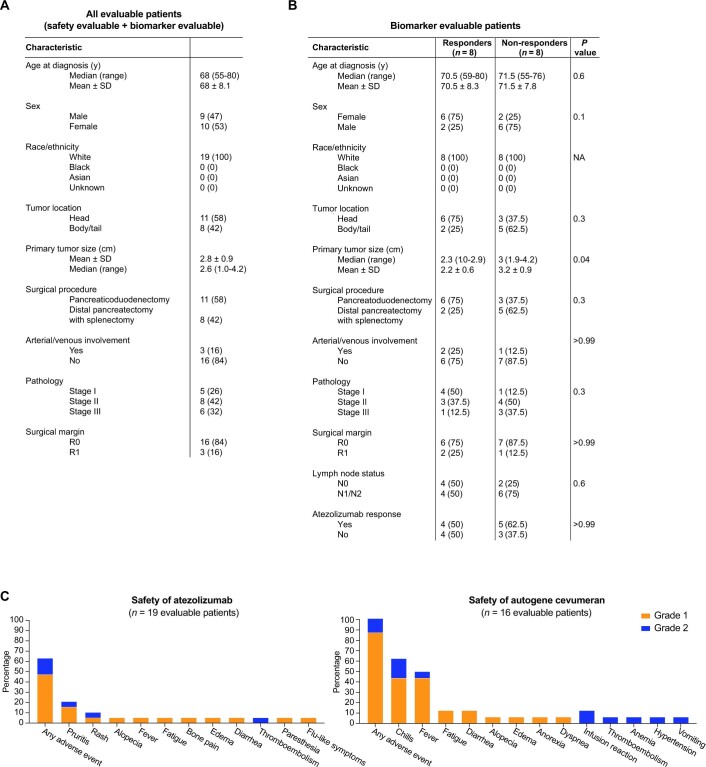
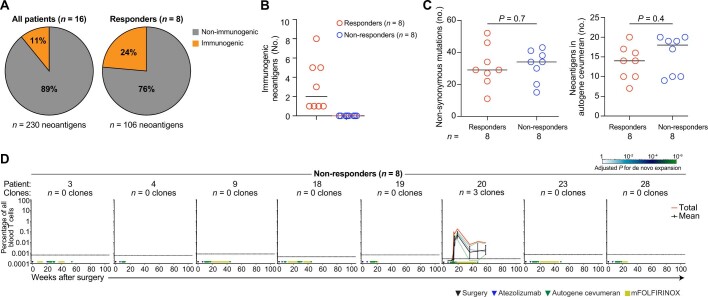
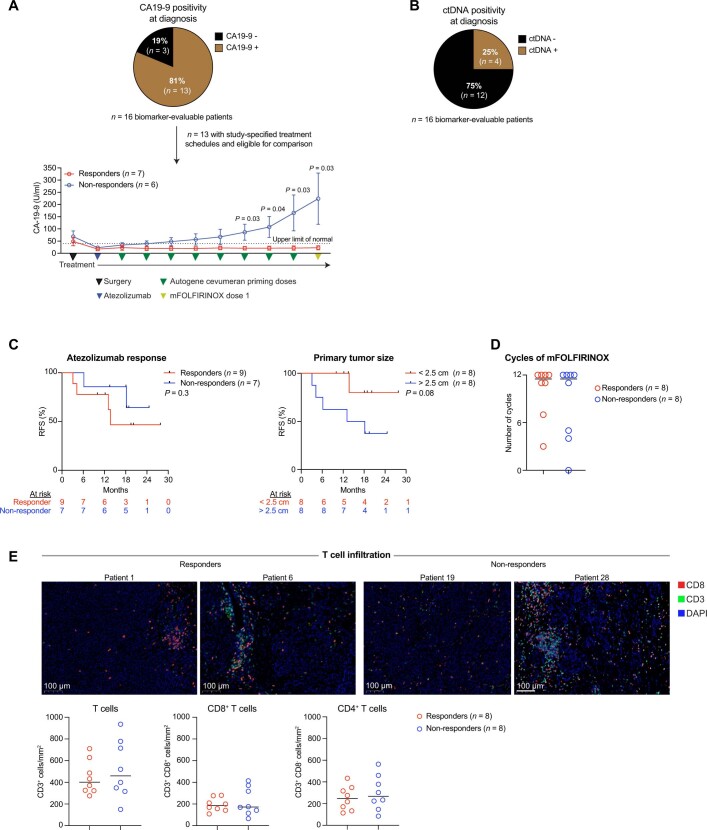
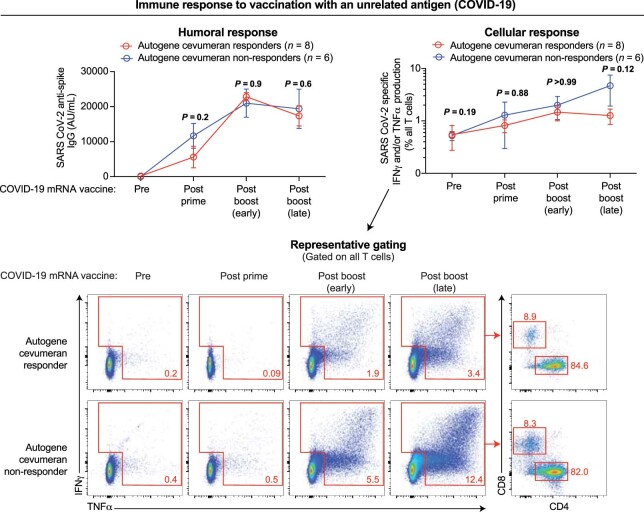
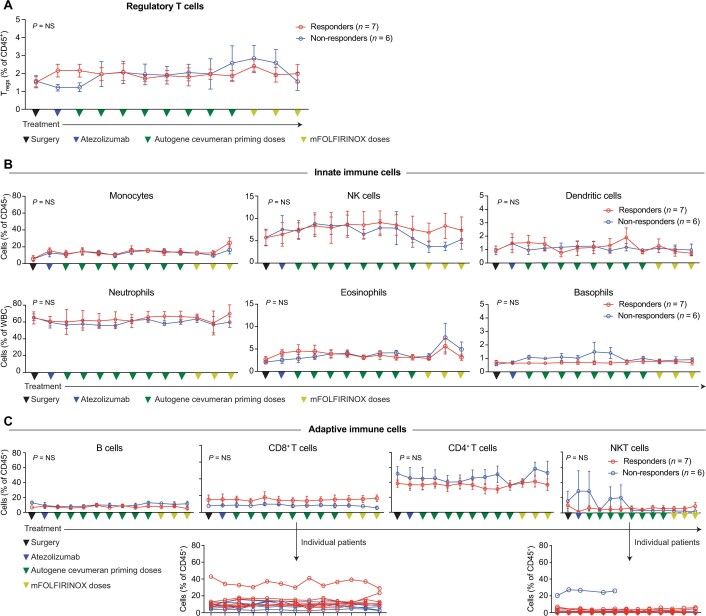
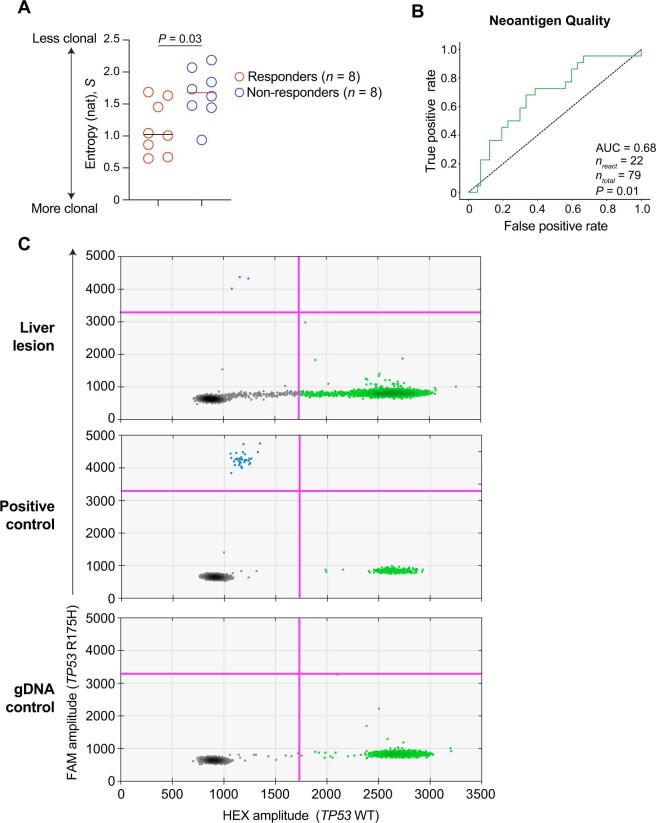
Pancreatic ductal adenocarcinoma (PDAC) is lethal in 88% of patients1, yet harbours mutation-derived T cell neoantigens that are suitable for vaccines 2,3. Here in a phase I trial of adjuvant autogene cevumeran, an individualized neoantigen vaccine based on uridine mRNA-lipoplex nanoparticles, we synthesized mRNA neoantigen vaccines in real time from surgically resected PDAC tumours. After surgery, we sequentially administered atezolizumab (an anti-PD-L1 immunotherapy), autogene cevumeran (a maximum of 20 neoantigens per patient) and a modified version of a four-drug chemotherapy regimen (mFOLFIRINOX, comprising folinic acid, fluorouracil, irinotecan and oxaliplatin). The end points included vaccine-induced neoantigen-specific T cells by high-threshold assays, 18-month recurrence-free survival and oncologic feasibility. We treated 16 patients with atezolizumab and autogene cevumeran, then 15 patients with mFOLFIRINOX. Autogene cevumeran was administered within 3 days of benchmarked times, was tolerable and induced de novo high-magnitude neoantigen-specific T cells in 8 out of 16 patients, with half targeting more than one vaccine neoantigen. Using a new mathematical strategy to track T cell clones (CloneTrack) and functional assays, we found that vaccine-expanded T cells comprised up to 10% of all blood T cells, re-expanded with a vaccine booster and included long-lived polyfunctional neoantigen-specific effector CD8+ T cells. At 18-month median follow-up, patients with vaccine-expanded T cells (responders) had a longer median recurrence-free survival (not reached) compared with patients without vaccine-expanded T cells (non-responders; 13.4 months, P = 0.003). Differences in the immune fitness of the patients did not confound this correlation, as responders and non-responders mounted equivalent immunity to a concurrent unrelated mRNA vaccine against SARS-CoV-2. Thus, adjuvant atezolizumab, autogene cevumeran and mFOLFIRINOX induces substantial T cell activity that may correlate with delayed PDAC recurrence.
© 2023. The Author(s).
Conflict of interest statement
L.A.R. is an inventor of a patent related to oncolytic viral therapy (US20170051022A1). L.A.R., Z.S., B.D.G. and V.P.B. are inventors on patent applications related to work on antigen cross-reactivity (PCT/US2023/011643) and tracking vaccine-expanded T cell clones. M.Ł., B.D.G. and V.P.B. are inventors on a patent application on neoantigen quality modelling (63/303,500). B.D.G. has received honoraria for speaking engagements from Merck, Bristol Meyers Squibb and Chugai Pharmaceuticals; has received research funding from Bristol Meyers Squibb, Merck, and ROME Therapeutics; and has been a compensated consultant for Darwin Health, Merck, PMV Pharma, Shennon Biotechnologies and Rome Therapeutics of which he is a co-founder. R.K.D. received one-time consulting fees from GE Healthcare and Bayer Healthcare. A.S.E. received royalties from Up-To-Date. A.M.V. discloses the following relationships (provision of services, uncompensated): Bristol-Myers Squibb, GlaxoSmithKline, Lilly Oncology, OBI Pharma, and Silenseed. M.S. has collaborative research agreements with Atara Biotherapeutics, Fate Therapeutics, Mnemo Therapeutics, and Takeda Pharmaceuticals. A.C.W. is a consultant for Histosonics and Biosapien; received honorarium from Medtronic and AstraZeneca; and received travel support from Intuitive Surgical. T.P.K. received a one-time consulting fee from Olympus Surgical. J.D. owns stock in Alnylam Pharmaceuticals, Arrowroot Acquisition, and Ionis Pharmaceuticals. W.P. receives grant and research support from Astellas, Merck, NIH/NCI, Parker Institute for Cancer Immunotherapy, and Break Through Cancer. E.M.O. receives grant and research support from Genentech/Roche, Celgene/Bristol-Myers Squibb, BioNTech, AstraZeneca, Arcus, Elicio, Parker Institute, and the NIH/NCI. T.M. is a co-founder and holds equity in IMVAQ Therapeutics; he is a consultant for Immunos Therapeutics, ImmunoGenesis and Pfizer; he has research support from Bristol-Myers Squibb, Surface Oncology, Kyn Therapeutics, Infinity Pharmaceuticals, Peregrine Pharmaceuticals, Adaptive Biotechnologies, Leap Therapeutics and Aprea; he has patents on applications related to work on oncolytic viral therapy, alphavirus-based vaccine, neoantigen modelling, CD40, GITR, OX40, PD-1 and CTLA-4. J.D.W. is a consultant for Apricity, CellCarta, Ascentage Pharma; AstraZeneca, Bicara Therapeutics, Boehringer Ingelheim, Bristol-Myers Squibb, Daiichi Sankyo, Dragonfly, Georgiamune, Imvaq, Larkspur, Psioxus, Recepta, Tizona, and Sellas. J.D.W. receives grant and research support from Bristol-Myers Squibb and Sephora. J.D.W. has equity in Apricity, Arsenal IO, Ascentage, Imvaq, Linneaus, Georgiamune, Maverick, and Tizona Therapeutics. V.P.B. has received honoraria for speaking engagements from Genentech, and research support from Bristol-Myers Squibb and Genentech. Ö.T. and U.S. are co-founders, management board members and employees at BioNTech. E.D. and F.M. are employees at BioNTech. I.R., M.Y. and I.M. are employees at Genentech. The other authors (K.C.S., C.O., N.P., E.P., J.L., N. Ceglia, P.G., A.C., R.Y., A.K.C., T.W., J.R., M.A., A.Z., Z.O., G.P., A. Dobrin, N. Cohen, L.T., O.B., M.G., S.K., P.M., E.W., R.S., A. Desai, M.I.D. and W.R.J.) declare no competing interests.
Figures




Comment in
-
Personalized mRNA Vaccine Immunogenic against PDAC.Cancer Discov. 2023 Jul 7;13(7):1504. doi: 10.1158/2159-8290.CD-NB2023-0038. Cancer Discov. 2023. PMID: 37163684
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
