

Confidence-based laboratory test reduction recommendation algorithm
- PMID: 37165369
- PMCID: PMC10173656
- DOI: 10.1186/s12911-023-02187-3
Confidence-based laboratory test reduction recommendation algorithm
Abstract
Background: We propose a new deep learning model to identify unnecessary hemoglobin (Hgb) tests for patients admitted to the hospital, which can help reduce health risks and healthcare costs.
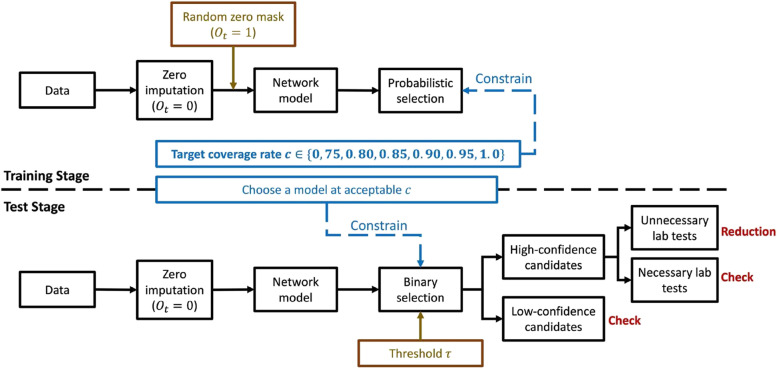
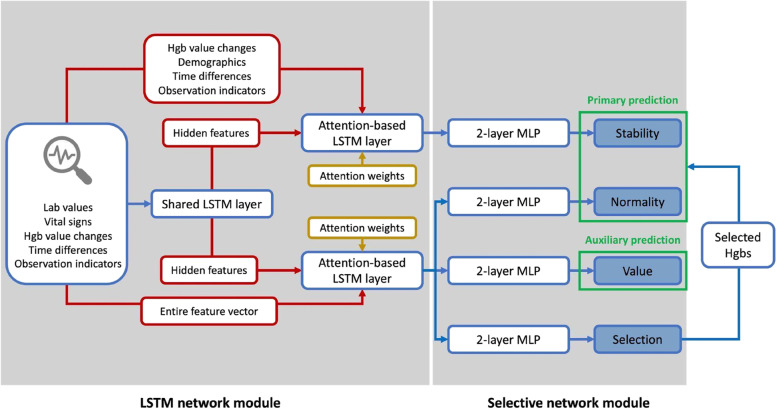
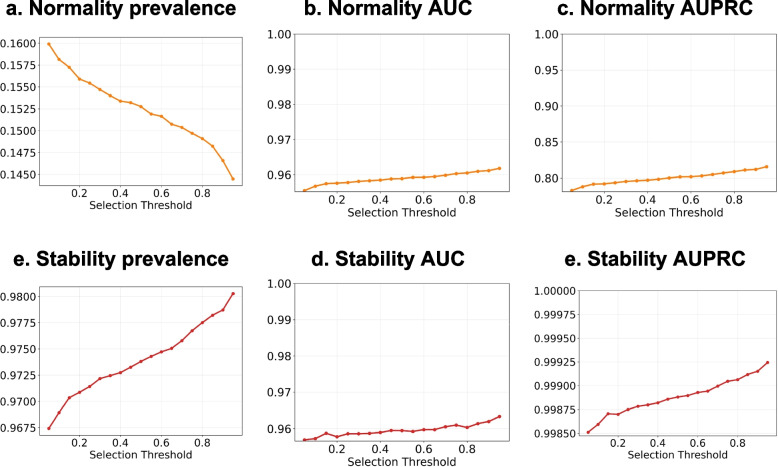
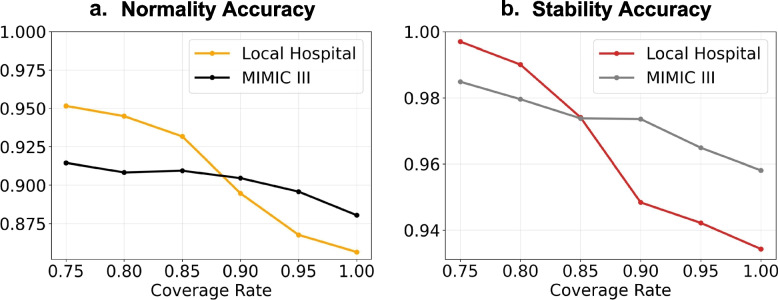
Methods: We collected internal patient data from a teaching hospital in Houston and external patient data from the MIMIC III database. The study used a conservative definition of unnecessary laboratory tests, which was defined as stable (i.e., stability) and below the lower normal bound (i.e., normality). Considering that machine learning models may yield less reliable results when trained on noisy inputs containing low-quality information, we estimated prediction confidence to assess the reliability of predicted outcomes. We adopted a "select and predict" design philosophy to maximize prediction performance by selectively considering samples with high prediction confidence for recommendations. Our model accommodated irregularly sampled observational data to make full use of variable correlations (i.e., with other laboratory test values) and temporal dependencies (i.e., previous laboratory tests performed within the same encounter) in selecting candidates for training and prediction.
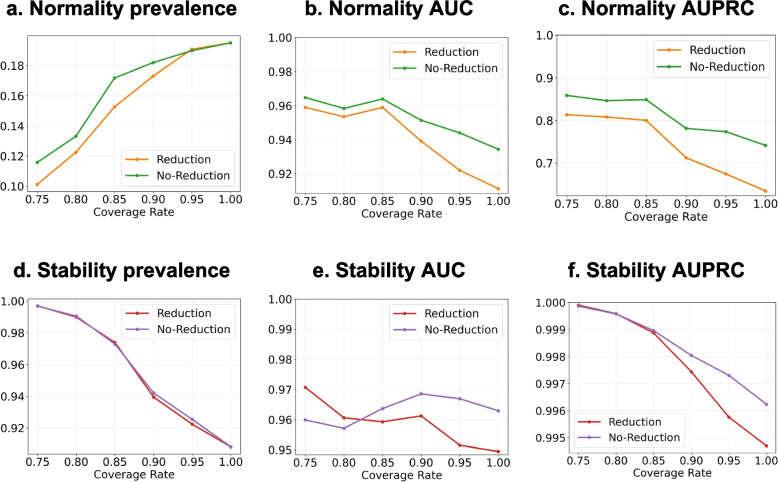
Results: The proposed model demonstrated remarkable Hgb prediction performance, achieving a normality AUC of 95.89% and a Hgb stability AUC of 95.94%, while recommending a reduction of 9.91% of Hgb tests that were deemed unnecessary. Additionally, the model could generalize well to external patients admitted to another hospital.
Conclusions: This study introduces a novel deep learning model with the potential to significantly reduce healthcare costs and improve patient outcomes by identifying unnecessary laboratory tests for hospitalized patients.
Keywords: Confidence based; Deep learning; Lab test reduction.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Does the Presence of Missing Data Affect the Performance of the SORG Machine-learning Algorithm for Patients With Spinal Metastasis? Development of an Internet Application Algorithm.Clin Orthop Relat Res. 2024 Jan 1;482(1):143-157. doi: 10.1097/CORR.0000000000002706. Epub 2023 Jun 12. Clin Orthop Relat Res. 2024. PMID: 37306629 Free PMC article.
-
Comparison of Two Modern Survival Prediction Tools, SORG-MLA and METSSS, in Patients With Symptomatic Long-bone Metastases Who Underwent Local Treatment With Surgery Followed by Radiotherapy and With Radiotherapy Alone.Clin Orthop Relat Res. 2024 Dec 1;482(12):2193-2208. doi: 10.1097/CORR.0000000000003185. Epub 2024 Jul 23. Clin Orthop Relat Res. 2024. PMID: 39051924
-
Are Current Survival Prediction Tools Useful When Treating Subsequent Skeletal-related Events From Bone Metastases?Clin Orthop Relat Res. 2024 Sep 1;482(9):1710-1721. doi: 10.1097/CORR.0000000000003030. Epub 2024 Mar 22. Clin Orthop Relat Res. 2024. PMID: 38517402
-
The effect of sample site and collection procedure on identification of SARS-CoV-2 infection.Cochrane Database Syst Rev. 2024 Dec 16;12(12):CD014780. doi: 10.1002/14651858.CD014780. Cochrane Database Syst Rev. 2024. PMID: 39679851 Free PMC article.
-
Interventions for implementation of thromboprophylaxis in hospitalized patients at risk for venous thromboembolism.Cochrane Database Syst Rev. 2018 Apr 24;4(4):CD008201. doi: 10.1002/14651858.CD008201.pub3. Cochrane Database Syst Rev. 2018. PMID: 29687454 Free PMC article.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
