Retinal arterial Aβ40 deposition is linked with tight junction loss and cerebral amyloid angiopathy in MCI and AD patients
- PMID: 37166032
- PMCID: PMC10638467
- DOI: 10.1002/alz.13086
Retinal arterial Aβ40 deposition is linked with tight junction loss and cerebral amyloid angiopathy in MCI and AD patients
Abstract
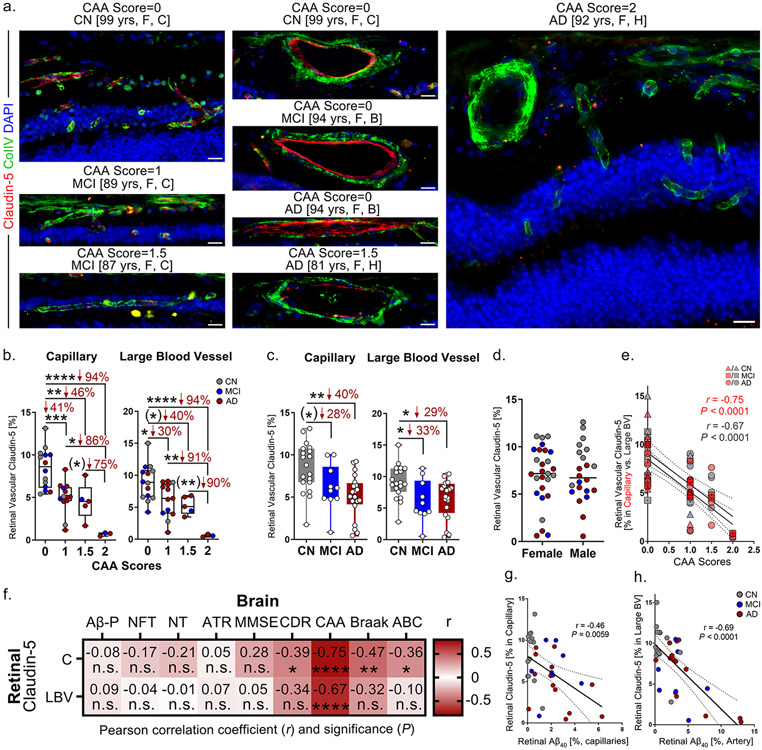
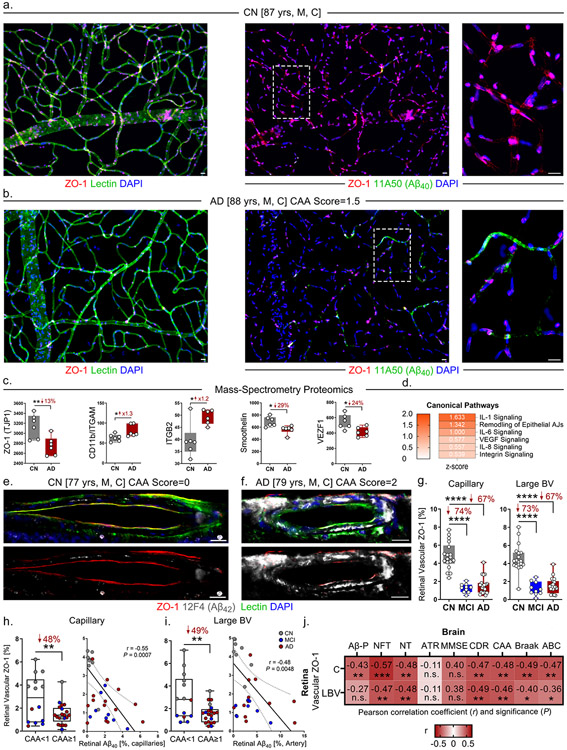
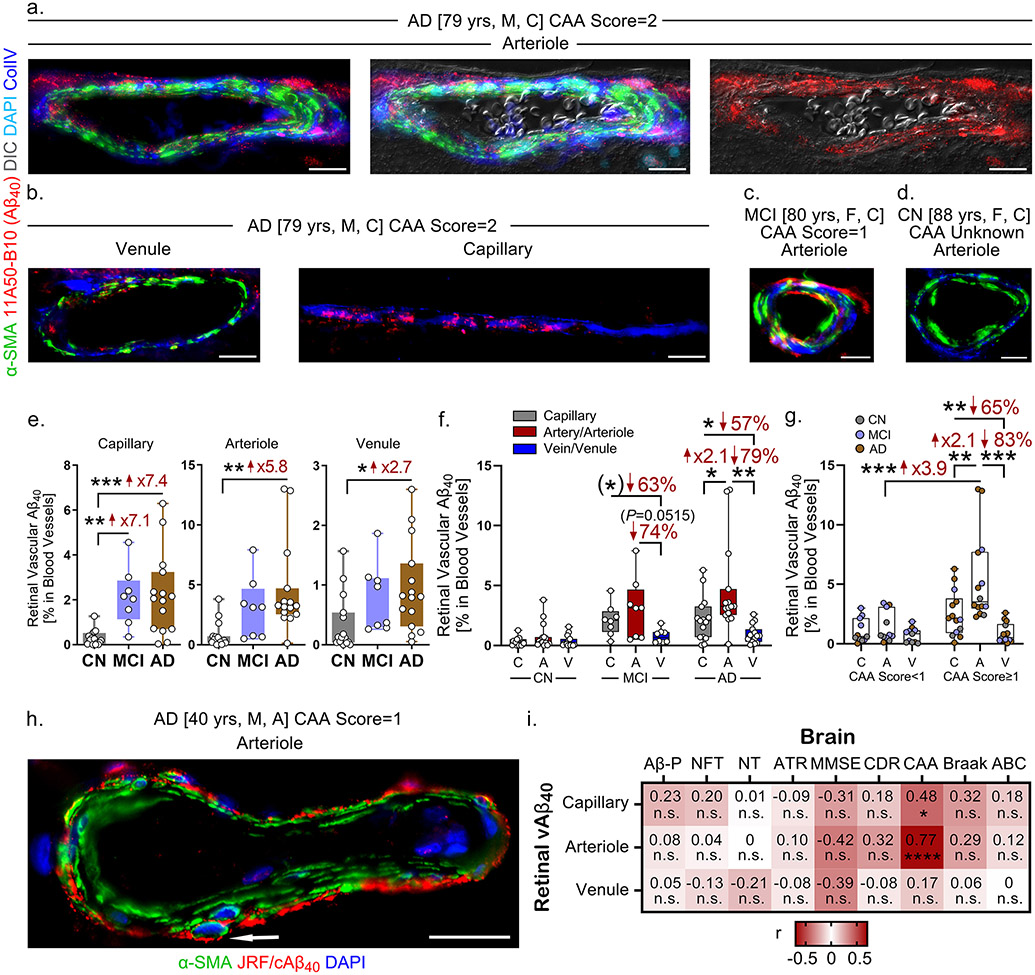
Introduction: Vascular amyloid beta (Aβ) protein deposits were detected in retinas of mild cognitively impaired (MCI) and Alzheimer's disease (AD) patients. We tested the hypothesis that the retinal vascular tight junctions (TJs) were compromised and linked to disease status.
Methods: TJ components and Aβ expression in capillaries and larger blood vessels were determined in post mortem retinas from 34 MCI or AD patients and 27 cognitively normal controls and correlated with neuropathology.
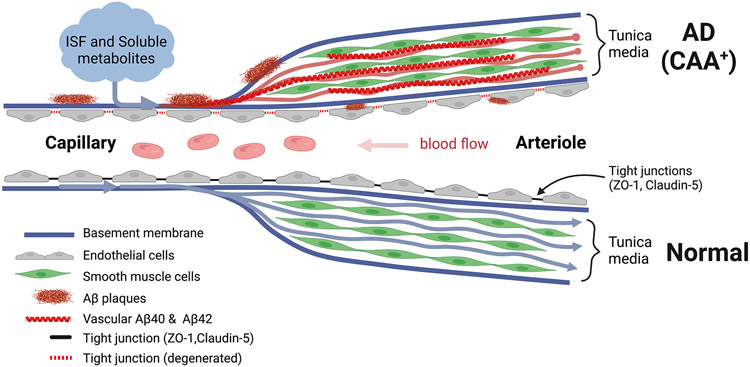
Results: Severe decreases in retinal vascular zonula occludens-1 (ZO-1) and claudin-5 correlating with abundant arteriolar Aβ40 deposition were identified in MCI and AD patients. Retinal claudin-5 deficiency was closely associated with cerebral amyloid angiopathy, whereas ZO-1 defects correlated with cerebral pathology and cognitive deficits.
Discussion: We uncovered deficiencies in blood-retinal barrier markers for potential retinal imaging targets of AD screening and monitoring. Intense retinal arteriolar Aβ40 deposition suggests a common pathogenic mechanism of failed Aβ clearance via intramural periarterial drainage.
Keywords: Alzheimer's disease; amyloid angiopathy; blood-retinal barrier; retinopathy.
© 2023 The Authors. Alzheimer's & Dementia published by Wiley Periodicals LLC on behalf of Alzheimer's Association.
Conflict of interest statement
Figures