

Assessment of Stool DNA Markers to Detect Colorectal Neoplasia in Patients with Inflammatory Bowel Disease: A Multi-site Case-control Study
- PMID: 37166153
- PMCID: PMC10588779
- DOI: 10.1093/ecco-jcc/jjad069
Assessment of Stool DNA Markers to Detect Colorectal Neoplasia in Patients with Inflammatory Bowel Disease: A Multi-site Case-control Study
Abstract
Background and aims: The FDA-approved multitarget stool-DNA [mt-sDNA] test is a successful colorectal cancer [CRC] screening tool in average-risk individuals but is not indicated for patients with inflammatory bowel disease [IBD]. We determined the performance of the mt-sDNA assay without the haemoglobin component [mt-sDNAHgb-] in patients with IBD, while measuring sensitivity for colorectal cancer and advanced colorectal neoplasia [ACRN].
Methods: This was a multi-centre, proof-of-concept investigation in persons aged 18-84 years with a diagnosis of IBD, or primary sclerosing cholangitis [PSC] with IBD. Enrolment occurred between March 2013 and May 2016. Stool was tested with the mt-sDNA molecular markers only, minus the immunochemical haemoglobin component.
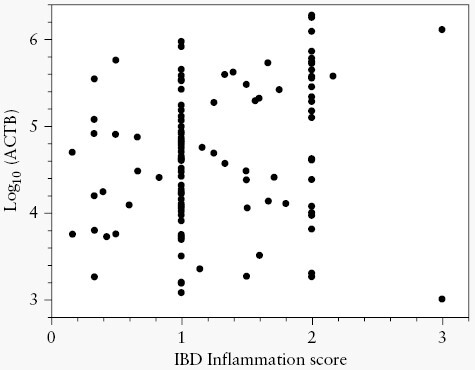
Results: The analysis set contained 355 samples. The median age was 52 [range 39-62] years, 45.6% were female and 93% were White. Two-thirds [63%] had ulcerative colitis [UC] and 10.1% had PSC/IBD. Colonoscopy revealed cancer in 8.5% [N = 30], advanced precancerous lesions [APLs] in 9.3% [N = 33] and non-advanced precancerous lesions in 7.6% [N = 27], and three-quarters [74.7%, N = 265] had negative findings. mt-sDNAHgb- sensitivity was 73.3% for any stage cancers, and 76.2% for ACRN. Sensitivity was highest for IBD-associated high-grade dysplasia at 100% and 84.6% for IBD-associated low-grade dysplasia ≥1 cm. The test showed higher sensitivity and lower specificity in UC than in Crohn's disease. Increasing inflammation score was associated with a significant decrease in mt-sDNAHgb- test score [ = 0.028] amongst neoplasia-negative individuals, but not in patients with ACRN.
Conclusions: These data highlight the potential of multitarget stool-DNA marker testing as an important addition to colorectal cancer surveillance by complementing colonoscopic evaluations in IBD patients.
Keywords: Colorectal neoplasms/prevention and control; inflammatory bowel diseases; stool/liquid biopsy.
© The Author(s) 2023. Published by Oxford University Press on behalf of European Crohn’s and Colitis Organisation.
Conflict of interest statement
Employment and disclosures: SI has received consulting fees and research support from Exact Sciences Corporation, research support from Freenome, and consulting fees from Geneoscopy. Mayo Clinic and Exact Sciences own intellectual property under which JBK is listed as an inventor and may receive royalties in accordance with Mayo Clinic policy. ZG, MO, JZ and MK are employees and shareholders of Exact Sciences. FAF has no relevant conflicts. PJL serves as Chief Medical Officer for Exact Sciences, initially through a contracted services agreement with Mayo Clinic [under which he and Mayo Clinic had contractual rights to receive royalties] and later as an Exact Sciences employee. The authors have no other relevant financial or non-financial interests to disclose.
Figures



References
-
- Laine L, Kaltenbach T, Barkun A, McQuaid KR, Subramanian V, Soetikno R; SCENIC Guideline Development Panel. SCENIC Guideline Development Panel. SCENIC international consensus statement on surveillance and management of dysplasia in inflammatory bowel disease. Gastrointest Endosc 2015;81:489–501.e26. doi: 10.1016/J.GIE.2014.12.009. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
