

Ultrasound imaging of the axilla
- PMID: 37166516
- PMCID: PMC10175532
- DOI: 10.1186/s13244-023-01430-9
Ultrasound imaging of the axilla
Abstract
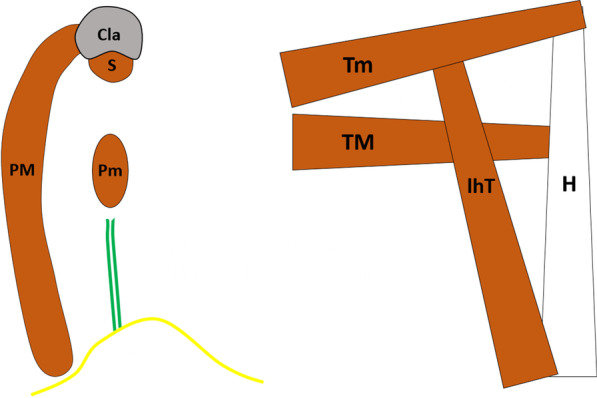
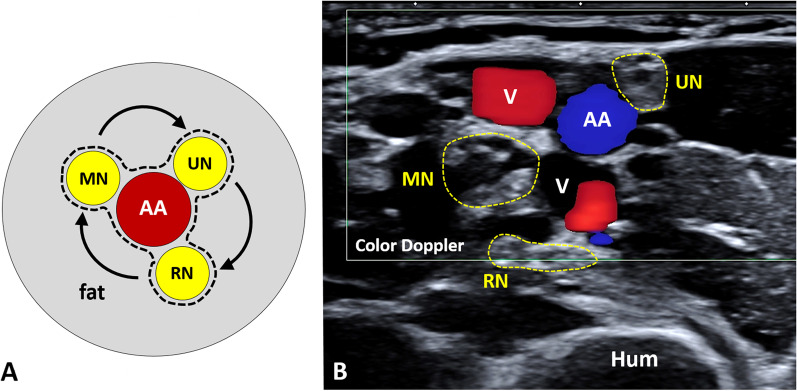
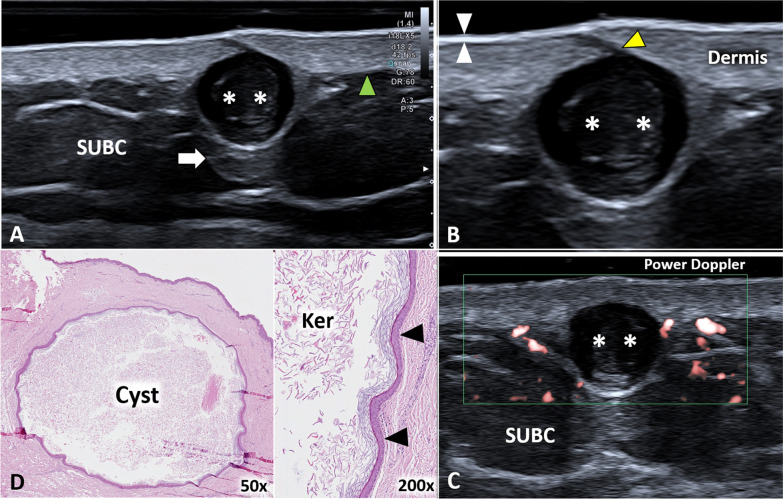
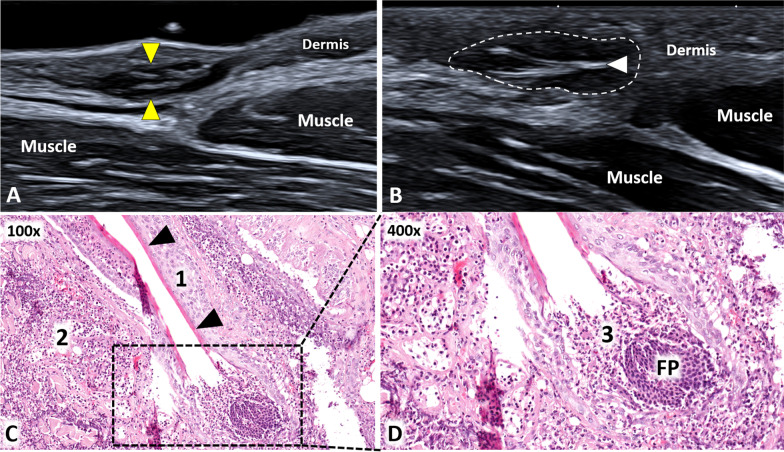
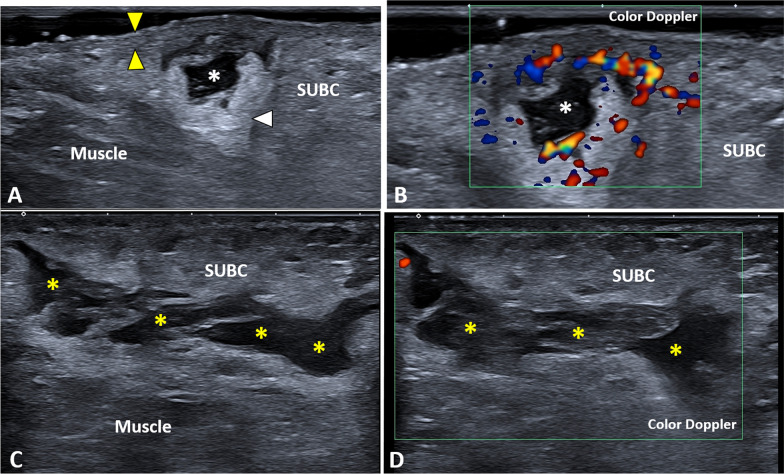
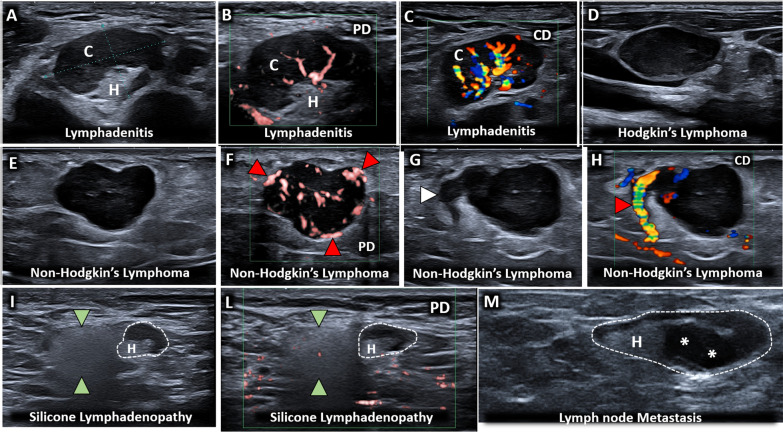
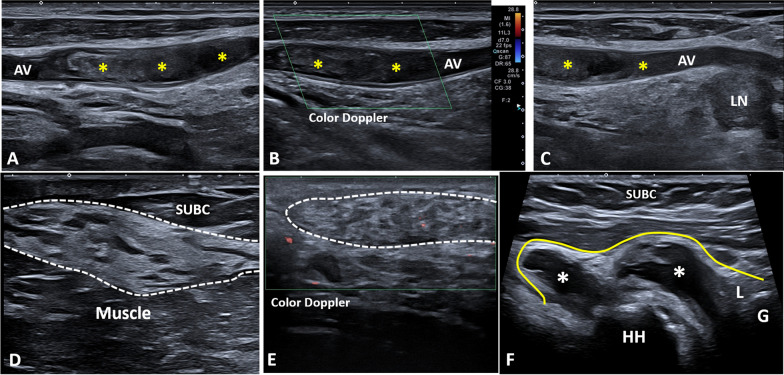
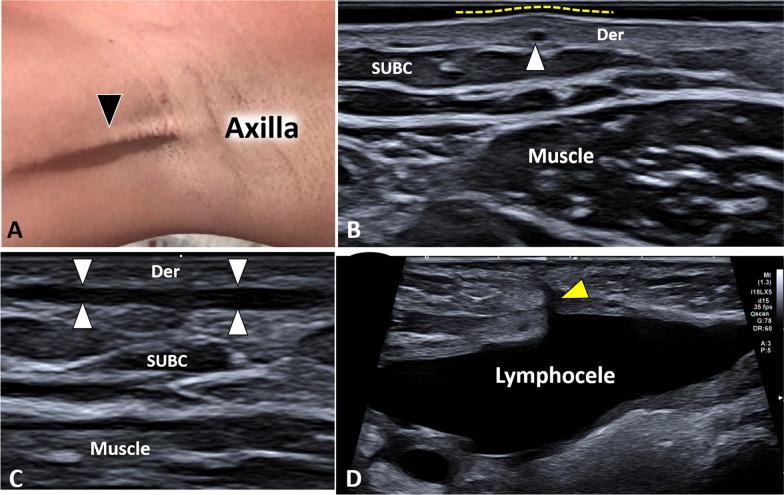
Axilla is a pyramidal-in-shape "virtual cavity" housing multiple anatomical structures and connecting the upper limb with the trunk. To the best of our knowledge, in the pertinent literature, a detailed sonographic protocol to comprehensively assess the axillary region in daily practice is lacking. In this sense, the authors have briefly described the anatomical architecture of the axilla-also using cadaveric specimens-to propose a layer-by-layer sonographic approach to this challenging district. The most common sonographic pathological findings-for each and every anatomical compartment of the axilla-have been accurately reported and compared with the corresponding histopathological features. This ultrasound approach could be considered a ready-to-use educational guidance for the assessment of the axillary region. CRITICAL RELEVANCE STATEMENT: Axilla is a pyramidal-in-shape "virtual cavity" housing multiple anatomical structures and connecting the upper limb with the trunk. The aim of this review article was to describe the anatomical architecture of the axilla, also using cadaveric specimens, in order to propose a layer-by-layer sonographic approach to this challenging district.
Keywords: Axilla; Histopathology; Ultrasound.
© 2023. The Author(s).
Conflict of interest statement
ADP and AC are members of the Insights into Imaging Editorial Board. They have not taken part in the review or selection process of this article. All remaining authors state no conflict of interest.
Figures




References
Publication types
LinkOut - more resources
Full Text Sources
Medical
