

Predicting preterm births from electrohysterogram recordings via deep learning
- PMID: 37167222
- PMCID: PMC10174487
- DOI: 10.1371/journal.pone.0285219
Predicting preterm births from electrohysterogram recordings via deep learning
Abstract
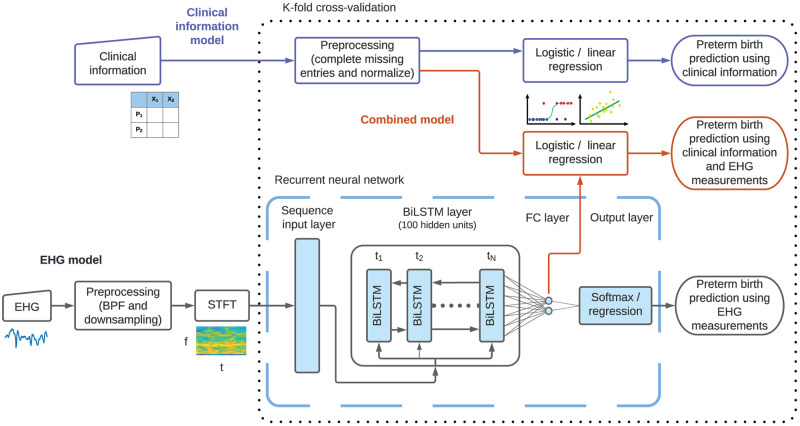
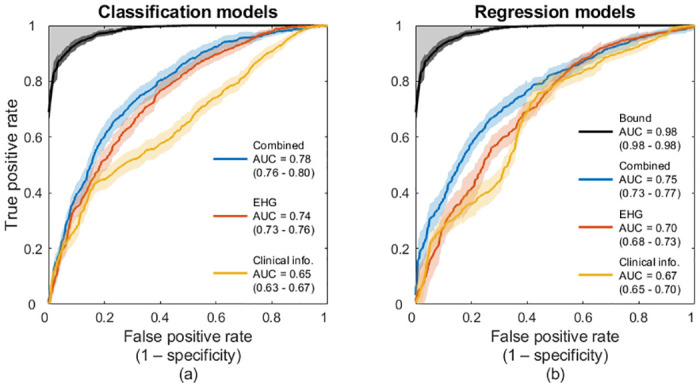
About one in ten babies is born preterm, i.e., before completing 37 weeks of gestation, which can result in permanent neurologic deficit and is a leading cause of child mortality. Although imminent preterm labor can be detected, predicting preterm births more than one week in advance remains elusive. Here, we develop a deep learning method to predict preterm births directly from electrohysterogram (EHG) measurements of pregnant mothers recorded at around 31 weeks of gestation. We developed a prediction model, which includes a recurrent neural network, to predict preterm births using short-time Fourier transforms of EHG recordings and clinical information from two public datasets. We predicted preterm births with an area under the receiver-operating characteristic curve (AUC) of 0.78 (95% confidence interval: 0.76-0.80). Moreover, we found that the spectral patterns of the measurements were more predictive than the temporal patterns, suggesting that preterm births can be predicted from short EHG recordings in an automated process. We show that preterm births can be predicted for pregnant mothers around their 31st week of gestation, prompting beneficial treatments to reduce the incidence of preterm births and improve their outcomes.
Copyright: © 2023 Goldsztejn, Nehorai. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

Similar articles
-
Electrohysterogram for ANN-Based Prediction of Imminent Labor in Women with Threatened Preterm Labor Undergoing Tocolytic Therapy.Sensors (Basel). 2020 May 8;20(9):2681. doi: 10.3390/s20092681. Sensors (Basel). 2020. PMID: 32397177 Free PMC article.
-
Enhancing classification of preterm-term birth using continuous wavelet transform and entropy-based methods of electrohysterogram signals.Front Endocrinol (Lausanne). 2023 Jan 10;13:1035615. doi: 10.3389/fendo.2022.1035615. eCollection 2022. Front Endocrinol (Lausanne). 2023. PMID: 36704040 Free PMC article.
-
Automatic semantic segmentation of EHG recordings by deep learning: An approach to a screening tool for use in clinical practice.Comput Methods Programs Biomed. 2024 Sep;254:108317. doi: 10.1016/j.cmpb.2024.108317. Epub 2024 Jul 5. Comput Methods Programs Biomed. 2024. PMID: 38996804
-
Electrohysterography in the diagnosis of preterm birth: a review.Physiol Meas. 2018 Feb 26;39(2):02TR01. doi: 10.1088/1361-6579/aaad56. Physiol Meas. 2018. PMID: 29406317 Review.
-
Accuracy of frequency-related parameters of the electrohysterogram for predicting preterm delivery: a review of the literature.Obstet Gynecol Surv. 2009 Aug;64(8):529-41. doi: 10.1097/OGX.0b013e3181a8c6b1. Obstet Gynecol Surv. 2009. PMID: 19624864 Review.
Cited by
-
Predicting risk of preterm birth in singleton pregnancies using machine learning algorithms.Front Big Data. 2024 Feb 29;7:1291196. doi: 10.3389/fdata.2024.1291196. eCollection 2024. Front Big Data. 2024. PMID: 38495848 Free PMC article.
-
An open dataset with electrohysterogram records of pregnancies ending in induced and cesarean section delivery.Sci Data. 2023 Oct 2;10(1):669. doi: 10.1038/s41597-023-02581-6. Sci Data. 2023. PMID: 37783671 Free PMC article.
-
Peak amplitude of the normalized power spectrum of the electromyogram of the uterus in the low frequency band is an effective predictor of premature birth.PLoS One. 2024 Sep 12;19(9):e0308797. doi: 10.1371/journal.pone.0308797. eCollection 2024. PLoS One. 2024. PMID: 39264880 Free PMC article.
References
-
- World Health Organization, et al. Born too soon: the global action report on preterm birth. 2012;.
MeSH terms
LinkOut - more resources
Full Text Sources
