

Characterising school-age health and function in rural Zimbabwe using the SAHARAN toolbox
- PMID: 37167268
- PMCID: PMC10174535
- DOI: 10.1371/journal.pone.0285570
Characterising school-age health and function in rural Zimbabwe using the SAHARAN toolbox
Abstract
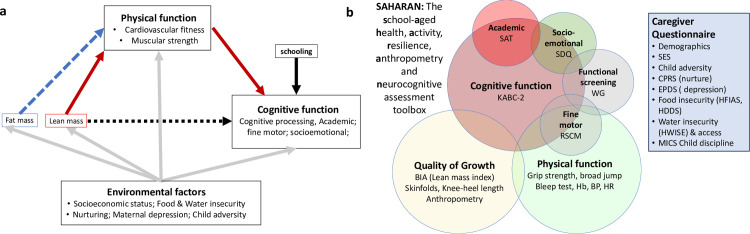
Introduction: We developed the School-Age Health, Activity, Resilience, Anthropometry and Neurocognitive (SAHARAN) toolbox to address the shortage of school-age assessment tools that combine growth, physical and cognitive function. Here we present i) development, acceptability and feasibility of the SAHARAN toolbox; ii) characteristics of a pilot cohort; and iii) associations between the domains measured in the cohort.
Methods: Growth was measured with anthropometry, knee-heel length and skinfold thicknesses. Bioimpedance analysis measured lean mass index and phase angle. Cognition was assessed using the mental processing index, derived from the Kaufman Assessment Battery for Children version 2, a fine motor finger-tapping task, and School Achievement Test (SAT). Physical function combined grip strength, broad jump and the 20m shuttle-run test to produce a total physical score. A caregiver questionnaire was performed in parallel.
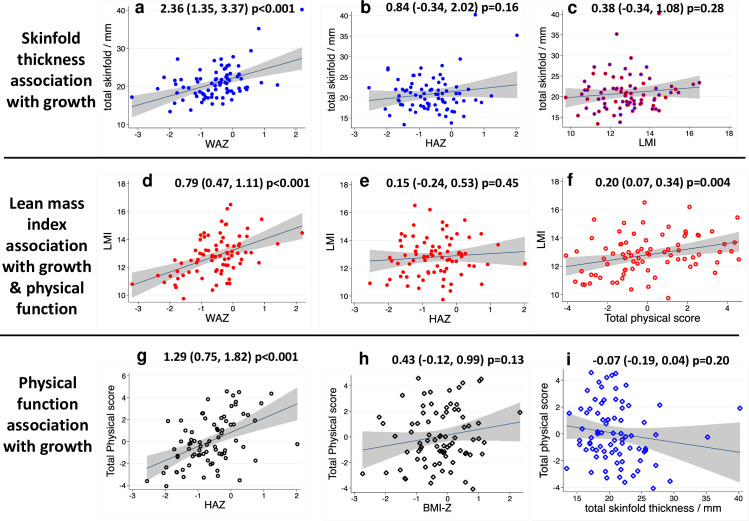
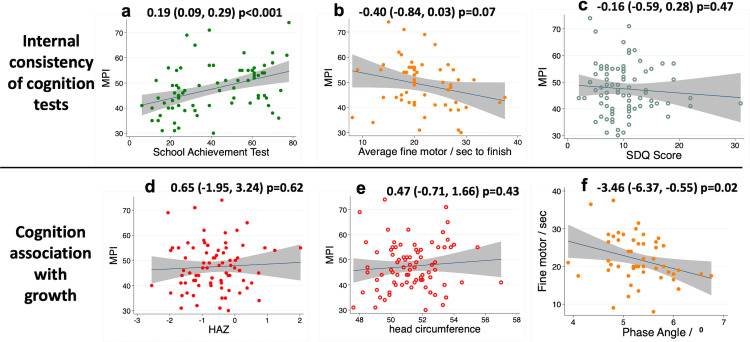
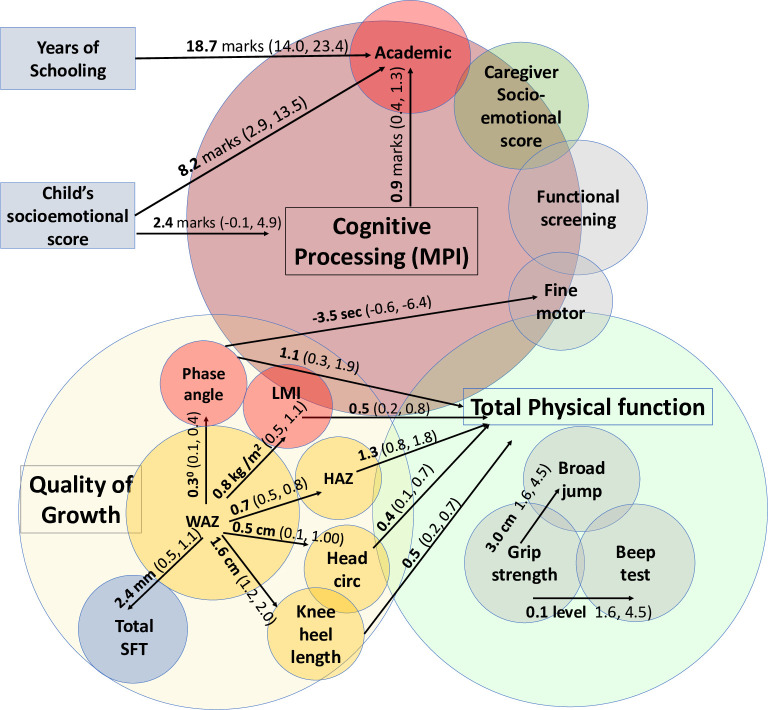
Results: The SAHARAN toolbox was feasible to implement in rural Zimbabwe, and highly acceptable to children and caregivers following some minor modifications. Eighty children with mean (SD) age 7.6 (0.2) years had mean height-for-age (HAZ) and weight-for-age Z-scores (WAZ) of -0.63 (0.81) and -0.55 (0.85), respectively. Lean mass index and total skinfold thicknesses were related to WAZ and BMI Z-score, but not to HAZ. Total physical score was associated with unit rises in HAZ (1.29, 95% CI 0.75, 1.82, p<0.001), and lean mass index (0.50, 95% CI 0.16, 0.83, p = 0.004), but not skinfold thicknesses. The SAT was associated with unit increases in the mental processing index and child socioemotional score. The caregiver questionnaire identified high levels of adversity and food insecurity.
Conclusions: The SAHARAN toolbox provided a feasible and acceptable holistic assessment of child growth and function in mid-childhood. We found clear associations between growth, height-adjusted lean mass and physical function, but not cognitive function. The SAHARAN toolbox could be deployed to characterise school-age growth, development and function elsewhere in sub-Saharan Africa.
Copyright: © 2023 Piper et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist
Figures
References
-
- WHO. The Global Strategy for Women’s, Children’s and Adolescents’ Health (2016–2030) 2015 [14/11/2019]. Available from: https://www.who.int/life-course/partners/global-strategy/global-strategy....
-
- WHO. Working Group 3: “Health in the missing middle (5–9 years) and early adolescence and Nutrition through the life-cycle”. 2020.
-
- Masquelier B, Hug L, Sharrow D, You D, Hogan D, Hill K, et al. Global, regional, and national mortality trends in older children and young adolescents from 1990 to 2016: an analysis of empirical data. The Lancet Global Health. 2018;6(10):e1087–e99. doi: 10.1016/S2214-109X(18)30353-X - DOI - PMC - PubMed
-
- Wibaek R, Vistisen D, Girma T, Admassu B, Abera M, Abdissa A, et al. Associations of fat mass and fat-free mass accretion in infancy with body composition and cardiometabolic risk markers at 5 years: The Ethiopian iABC birth cohort study. PLoS Med. 2019;16(8):e1002888. Epub 2019/08/21. doi: 10.1371/journal.pmed.1002888 ; PubMed Central PMCID: PMC6701744. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
