

Validation of a pre-established triage protocol for critically ill patients in a COVID-19 outbreak under resource scarcity: A retrospective multicenter cohort study
- PMID: 37167306
- PMCID: PMC10174588
- DOI: 10.1371/journal.pone.0285690
Validation of a pre-established triage protocol for critically ill patients in a COVID-19 outbreak under resource scarcity: A retrospective multicenter cohort study
Abstract
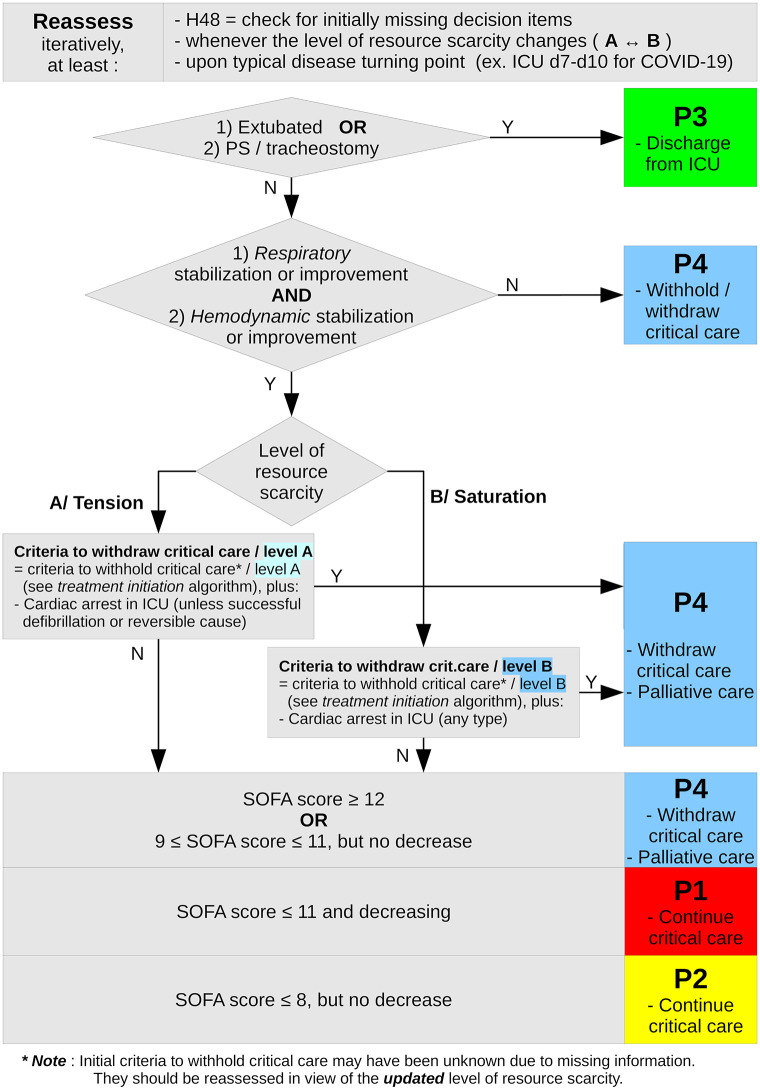
Introduction: In case of COVID-19 related scarcity of critical care resources, an early French triage algorithm categorized critically ill patients by probability of survival based on medical history and severity, with four priority levels for initiation or continuation of critical care: P1 -high priority, P2 -intermediate priority, P3 -not needed, P4 -not appropriate. This retrospective multi-center study aimed to assess its classification performance and its ability to help saving lives under capacity saturation.
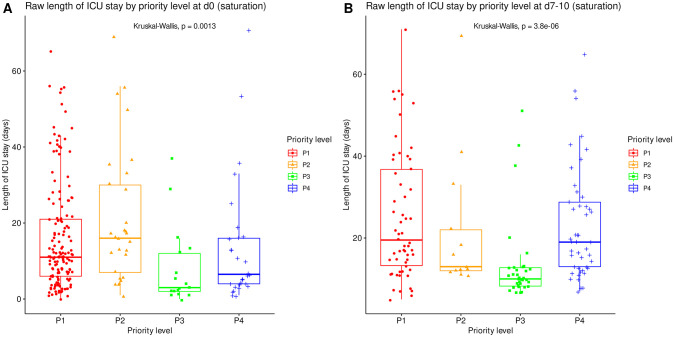
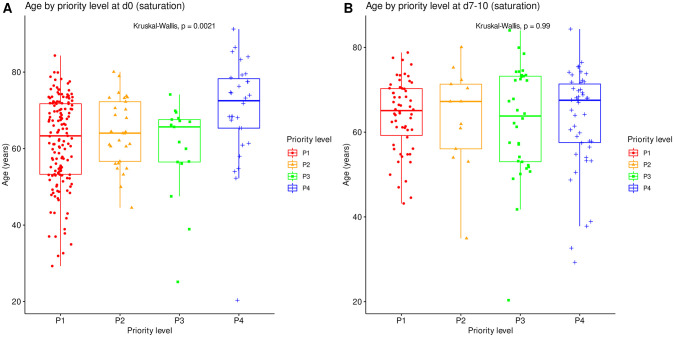
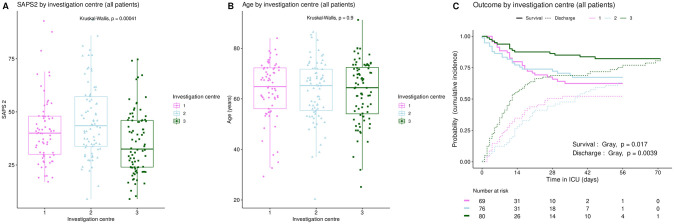
Methods: ICU patients admitted for severe COVID-19 without triage in spring 2020 were retrospectively included from three hospitals. Demographic data, medical history and severity items were collected. Priority levels were retrospectively allocated at ICU admission and on ICU day 7-10. Mortality rate, cumulative incidence of death and of alive ICU discharge, length of ICU stay and of mechanical ventilation were compared between priority levels. Calculated mortality and survival were compared between full simulated triage and no triage.
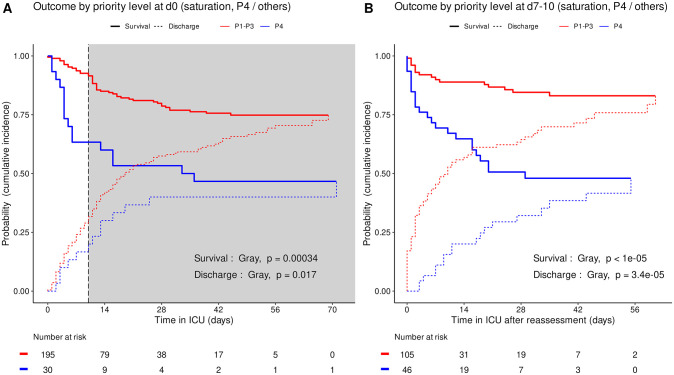
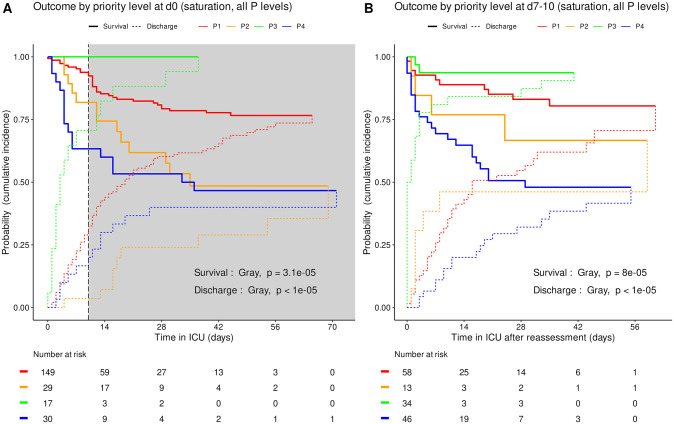
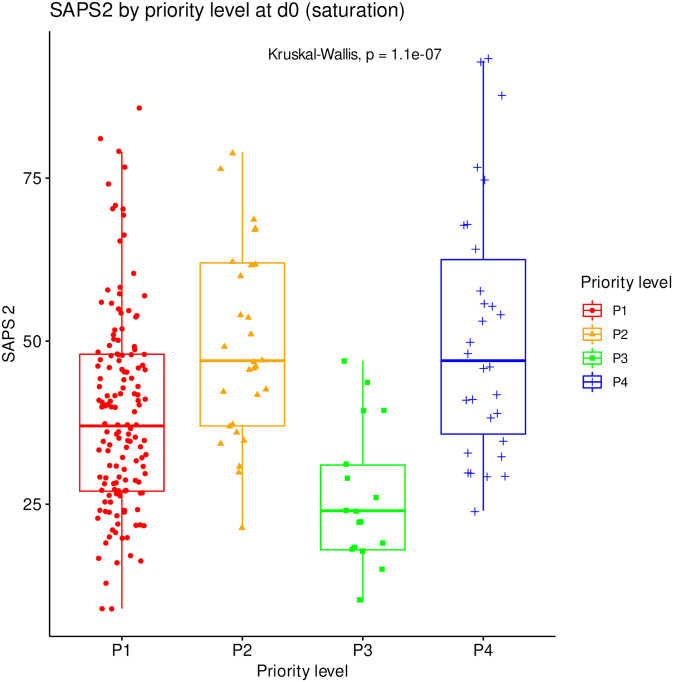
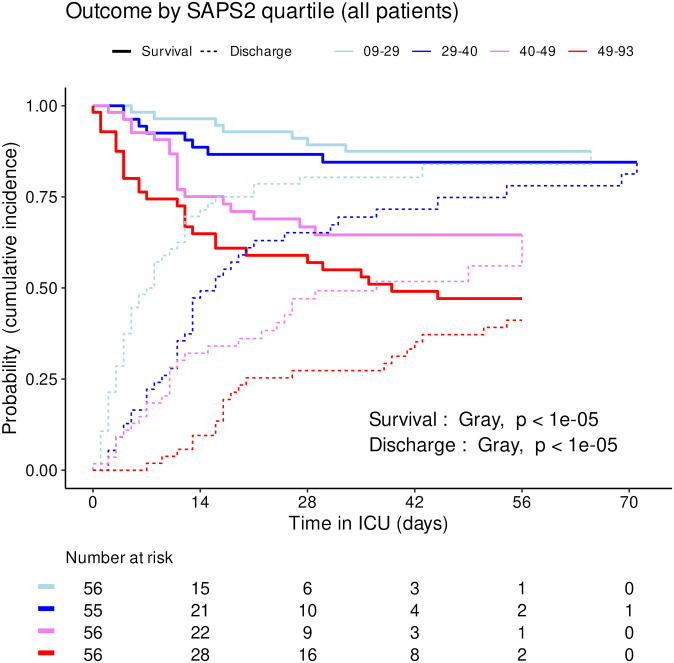
Results: 225 patients were included, aged 63.1±11.9 years. Median SAPS2 was 40 (IQR 29-49). At the end of follow-up, 61 (27%) had died, 26 were still in ICU, and 138 had been discharged. Following retrospective initial priority allocation, mortality rate was 53% among P4 patients (95CI 34-72%) versus 23% among all P1 to P3 patients (95CI 17-30%, chi-squared p = 5.2e-4). The cumulative incidence of death consistently increased in the order P3, P1, P2 and P4 both at admission (Gray's test p = 3.1e-5) and at reassessment (p = 8e-5), and conversely for that of alive ICU discharge. Reassessment strengthened consistency. Simulation under saturation showed that this two-step triage protocol could have saved 28 to 40 more lives than no triage.
Conclusion: Although it cannot eliminate potentially avoidable deaths, this triage protocol proved able to adequately prioritize critical care for patients with highest probability of survival, hence to save more lives if applied.
Copyright: © 2023 Donat et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures



References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
