

Beneficial effects of fecal microbiota transplantation in recurrent Clostridioides difficile infection
- PMID: 37167952
- PMCID: PMC10966711
- DOI: 10.1016/j.chom.2023.03.019
Beneficial effects of fecal microbiota transplantation in recurrent Clostridioides difficile infection
Abstract
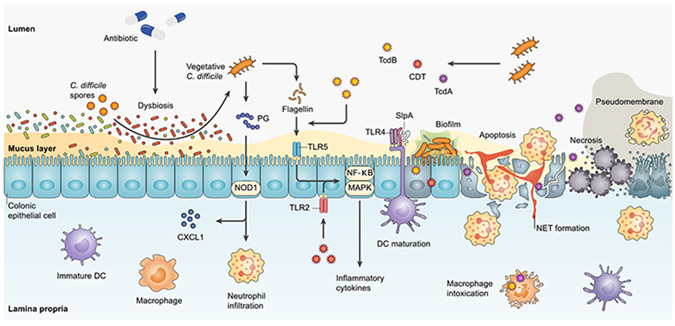
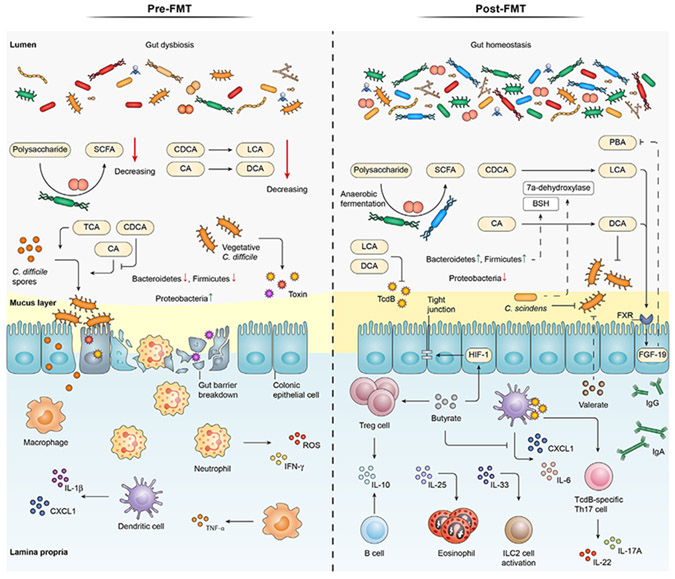
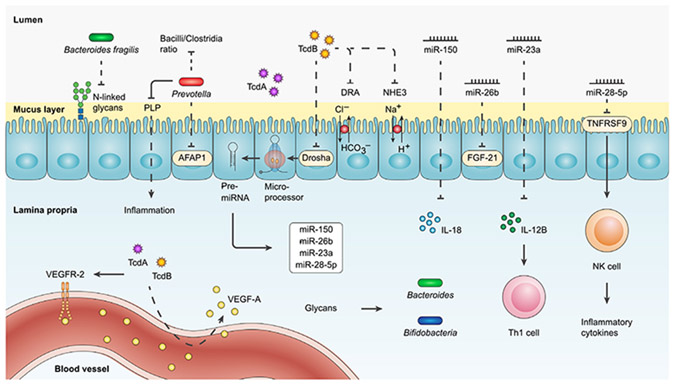
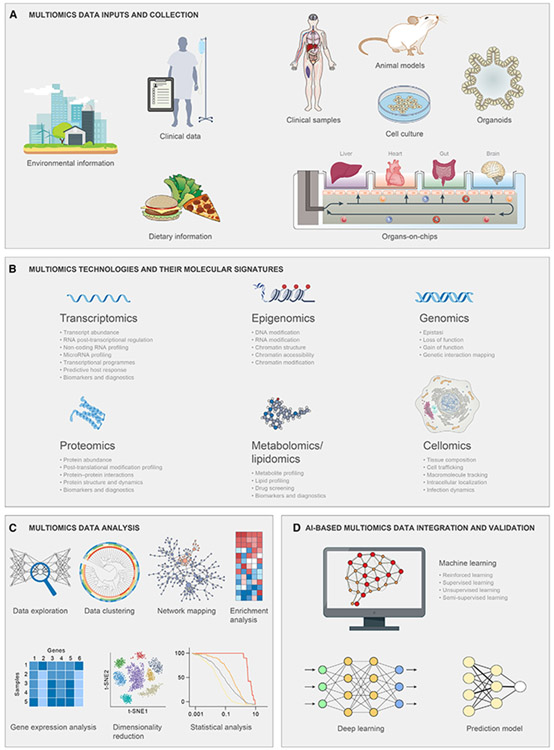
Fecal microbiota transplantation (FMT) is highly effective in preventing recurrent Clostridioides difficile infection (rCDI). However, the mechanisms underpinning its clinical efficacy are incompletely understood. Herein, we provide an overview of rCDI pathogenesis followed by a discussion of potential mechanisms of action focusing on the current understanding of trans-kingdom microbial, metabolic, immunological, and epigenetic mechanisms. We then outline the current research gaps and offer methodological recommendations for future studies to elevate the quality of research and advance knowledge translation. By combining interventional trials with multiomics technology and host and environmental factors, analyzing longitudinally collected biospecimens will generate results that can be validated with animal and other models. Collectively, this will confirm causality and improve translation, ultimately to develop targeted therapies to replace FMT.
Keywords: fecal microbiota transplantation; host-microbial interactions; intestinal microbial transfer; recurrent Clostridioides difficile infection.
Copyright © 2023 Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests D.K. has served on the adjudication board for Finch Therapeutics and has received consulting fees and a speaking honorarium from Rebiotix/Ferring Pharmaceuticals. A.M.S. has received consultation fees from Finch Therapeutics and Rebiotix/Ferring Pharmaceuticals.
Figures
References
-
- Johnson S, Lavergne V, Skinner AM, Gonzales-Luna AJ, Garey KW, Kelly CP, and Wilcox MH (2021). Clinical practice guideline by the Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA): 2021 focused update guidelines on management of Clostridioides difficile infection in adults. Clin. Infect. Dis 73, 755–757. - PubMed
-
- Fekety R, McFarland LV, Surawicz CM, Greenberg RN, Elmer GW, and Mulligan ME (1997). Recurrent Clostridium difficile diarrhea: characteristics of and risk factors for patients enrolled in a prospective, randomized, double-blinded trial. Clin. Infect. Dis 24, 324–333. - PubMed
-
- Keller JJ, and Kuijper EJ (2015). Treatment of recurrent and severe Clostridium difficile infection. Annu. Rev. Med 66, 373–386. - PubMed
-
- Dubberke ER, Lee CH, Orenstein R, Khanna S, Hecht G, and Gerding DN (2018). Results from a randomized, placebo-controlled clinical trial of a RBX2660-A microbiota-based drug for the prevention of recurrent Clostridium difficile infection. Clin. Infect. Dis 67, 1198–1204. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
