

Recurrent Meningitis After a Post-Traumatic Intradiploic Arachnoid Cyst: A Case Report
- PMID: 37168148
- PMCID: PMC10166393
- DOI: 10.7759/cureus.37124
Recurrent Meningitis After a Post-Traumatic Intradiploic Arachnoid Cyst: A Case Report
Abstract
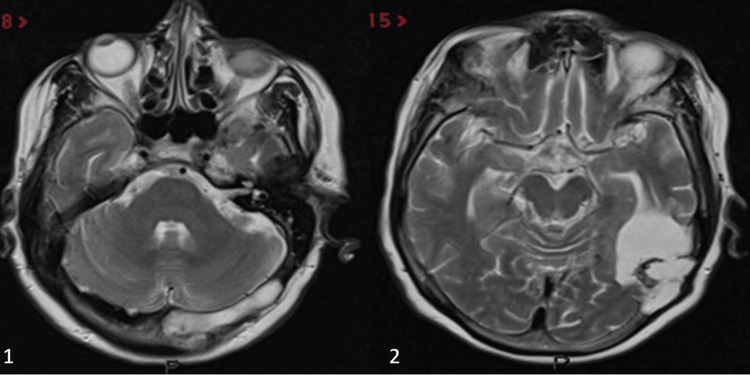
Intradiploic arachnoid cysts are infrequent but benign lesions of the central nervous system. Etiologically, they can be non-traumatic or post-traumatic in origin. We present an unusual case of a post-traumatic intradiploic arachnoid cyst presented with recurrent meningitis episodes. A 68-year-old female patient was admitted to the emergency department with fever and loss of consciousness, with a history of cranial operation due to a gunshot injury to the left occipital bone 45 years ago. On the patient's initial examination, nuchal rigidity was detected; Kernig's and Brudzinski's signs were positive. A lumbar puncture has been performed, and the patient is diagnosed with meningitis. The patient had been admitted to the emergency department with rhinorrhea after a minor blunt head trauma six years ago. As we understood from the patient's medical records, a couple of millimetric non-specified pneumocephalus areas, located next to the sella turcica, were detected on the cranial non-contrast-enhanced CT scan after the minor blunt trauma to the frontal bone. However, there was no sign of any obvious skull base fracture. The patient was hospitalized for five days and discharged on the sixth day without any complaints. After the discharge, the patient was admitted to other hospitals five times in the last five years with fever and anxiety. On all her admissions, the patient was diagnosed with CSF-culture-negative meningitis and treated with different unknown antibiotics. Magnetic resonance imaging (MRI) showed some irregularities and thinning at the inner table of the left occipital bone; there was an enlargement of the diploic distance of the occipital bone on the left side. MR cisternography showed cerebrospinal fluid (CSF) fistulizing areas just below the thickened and irregular part of the occipital bone. CSF fistula was communicated with the left lateral ventricle. The occipital horn of the left lateral ventricle was enlarged. We performed a surgical repair in order to cover the defective areas of the occipital and mastoid bones. The retromastoid approach was used. Pedunculated muscle flaps to cover the defective bony areas are used and secured with fibrin glue. There is no evidence of recurrence during the one-year follow-up period of the patient. We present this unusual case to emphasize that if post-traumatic intradiploic arachnoid cysts remain untreated, severe complications, such as episodes of recurrent meningitis, may occur. Although a few cases of these cysts are reported in the literature, a case of post-traumatic intradiploic arachnoid cyst presenting with recurrent meningitis has not been reported. In patients with recurrent meningitis, when no prominent etiology is found and if there is a trauma to the related bone in the patient's history, post-traumatic intradiploic arachnoid cyst should be included in the differential diagnosis.
Keywords: csf-culture negative meningitis; intradiploic arachnoid cyst; negative csf culture; post-traumatic intradiploic arachnoid cyst; recurrent meningitis.
Copyright © 2023, Yangi et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures


Similar articles
-
Post-Traumatic Occipital Intradiploic Encephalocele.World Neurosurg. 2019 Sep;129:9-12. doi: 10.1016/j.wneu.2019.05.174. Epub 2019 May 29. World Neurosurg. 2019. PMID: 31150845
-
Giant intradiploic arachnoid cyst for 13 years.J Pediatr Neurosci. 2014 May;9(2):139-41. doi: 10.4103/1817-1745.139318. J Pediatr Neurosci. 2014. PMID: 25250069 Free PMC article.
-
Intradiploic arachnoid cyst identified by diffusion-weighted magnetic resonance imaging--case report.Neurol Med Chir (Tokyo). 2002 Mar;42(3):137-9. doi: 10.2176/nmc.42.137. Neurol Med Chir (Tokyo). 2002. PMID: 11936057
-
Posttraumatic intradiploic arachnoid cyst of the posterior fossa.Childs Nerv Syst. 1997 May;13(5):293-6. doi: 10.1007/s003810050088. Childs Nerv Syst. 1997. PMID: 9224921 Review.
-
Post-traumatic intradiploic leptomeningeal fistula and cyst.J Clin Neurosci. 2002 Jul;9(4):468-73. doi: 10.1054/jocn.2002.1066. J Clin Neurosci. 2002. PMID: 12217685 Review.
References
-
- Leptomeningeal cyst of the posterior fossa. Case report. Dunkser SB, McCreary HS. J Neurosurg. 1971;34:687–692. - PubMed
-
- Intradiploic arachnoid cysts. Report of two cases. Weinand ME, Rengachary SS, McGregor DH, Watanabe I. J Neurosurg. 1989;70:954–958. - PubMed
-
- Giant intradiploic pseudomeningocele of occipital bone. Kumar R, Chandra SP, Sharma BS. J Neurosurg Pediatr. 2012;9:82–85. - PubMed
-
- Low-pressure headaches following foramen magnum decompression secondary to absorption of cerebrospinal fluid into the venous system of the diploic space. Bulleid LS, Hughes T, Bhatti I, Leach PA. Childs Nerv Syst. 2016;32:897–899. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials