

Metabolic genes, a potential predictor of prognosis and immunogenicity of clear cell renal cell carcinoma
- PMID: 37168330
- PMCID: PMC10164820
Metabolic genes, a potential predictor of prognosis and immunogenicity of clear cell renal cell carcinoma
Abstract
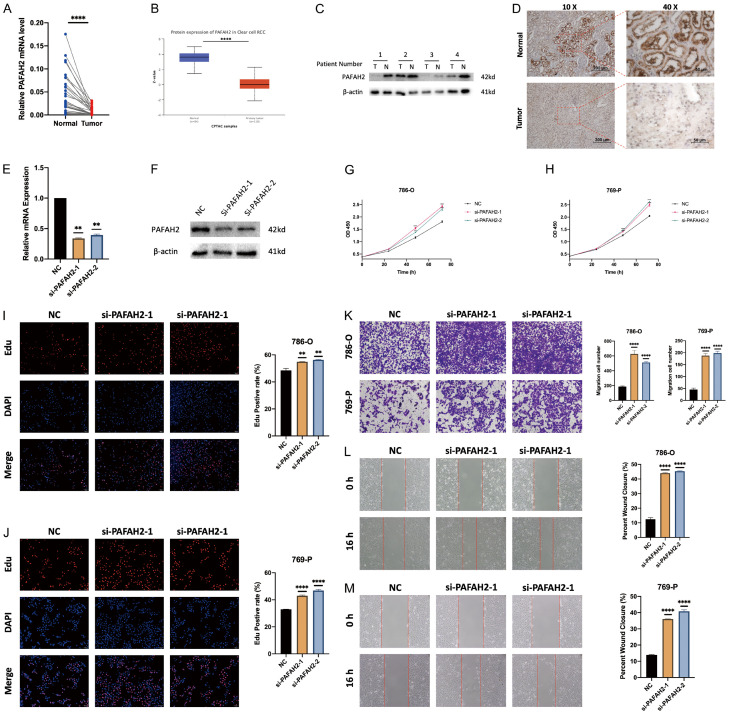
Clear cell renal cell carcinoma (ccRCC) is the most common subtype of renal cell carcinoma (RCC). Many ccRCCs are diagnosed at an advanced stage due to the lack of early symptoms, with a high mortality rate and a poor prognosis. The occurrence and development of ccRCC are closely related to metabolic disorders. This study aims to explore the relationship between metabolic genes and prognosis, immune microenvironment, and tumor development of ccRCC. Using data from TCGA, GEO, and ArrayExpress, we successfully established a risk model (riskScore) based on 4 metabolic genes (MGs) that can accurately predict the prognosis and immune microenvironment of ccRCCs. In addition, we determined the role of PAFAH2 in suppressing tumor cell proliferation and migration in ccRCC in vitro. Our research may shed new light on ccRCC patients' prognosis and treatment management.
Keywords: Metabolic genes; PAFAH2; TME; ccRCC; prognosis.
AJCR Copyright © 2023.
Conflict of interest statement
None.
Figures





References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2019. CA Cancer J Clin. 2019;69:7–34. - PubMed
-
- Hakimi AA, Voss MH, Kuo F, Sanchez A, Liu M, Nixon BG, Vuong L, Ostrovnaya I, Chen YB, Reuter V, Riaz N, Cheng Y, Patel P, Marker M, Reising A, Li MO, Chan TA, Motzer RJ. Transcriptomic profiling of the tumor microenvironment reveals distinct subgroups of clear cell renal cell cancer: data from a randomized phase III trial. Cancer Discov. 2019;9:510–525. - PMC - PubMed
-
- Choueiri TK, Motzer RJ. Systemic therapy for metastatic renal-cell carcinoma. N Engl J Med. 2017;376:354–366. - PubMed
-
- Capitanio U, Montorsi F. Renal cancer. Lancet. 2016;387:894–906. - PubMed
LinkOut - more resources
Full Text Sources