

Recanalization and outcomes after cerebral venous thrombosis: a systematic review and meta-analysis
- PMID: 37168399
- PMCID: PMC10165140
- DOI: 10.1016/j.rpth.2023.100143
Recanalization and outcomes after cerebral venous thrombosis: a systematic review and meta-analysis
Abstract
Background: Recanalization in cerebral venous thrombosis (CVT) can begin as early as 1 week after initiating therapeutic anticoagulation. The clinical significance of recanalization remains uncertain.
Objectives: We aimed to investigate the association between recanalization and functional outcomes and explored predictors of recanalization.
Methods: A systematic literature search was conducted (EMBASE, MEDLINE, Cochrane library) to identify: (1) patients with CVT aged ≥18 years treated with anticoagulation only; (2) case series, cohort, or randomized controlled trial studies; and (3) reported recanalization rates and functional outcomes using either a modified Rankin Scale (mRS) or sequelae of CVT at last follow-up. Meta-analysis was performed using pooled odds ratios (ORs) with exploration of sex and age effects using meta-regression.
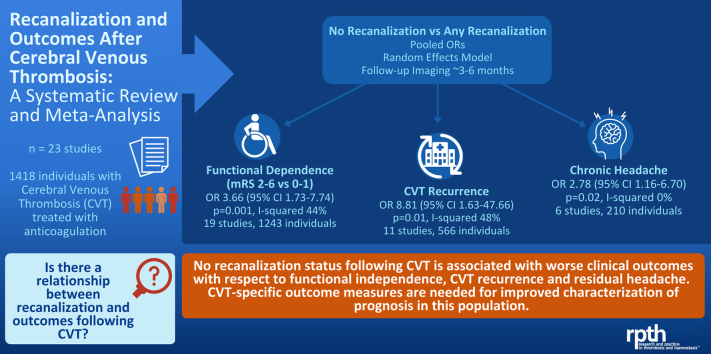
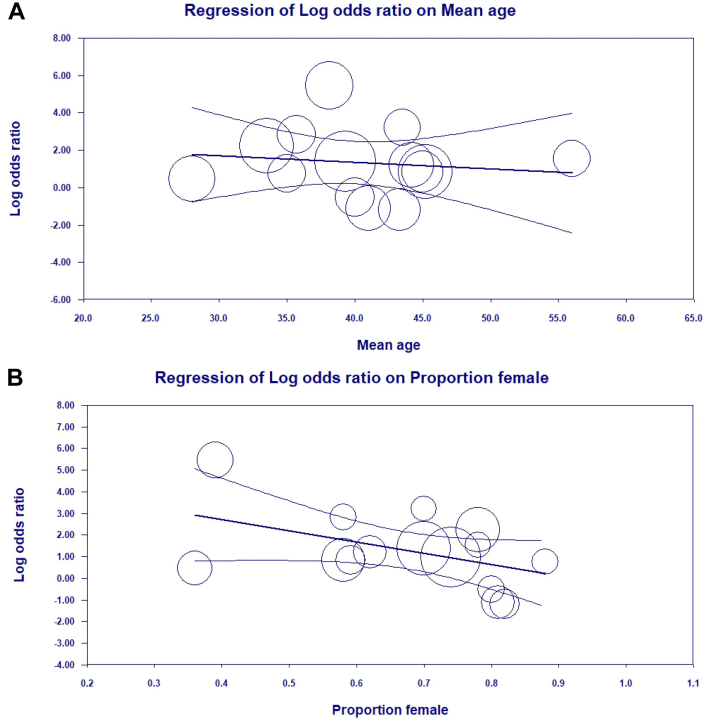
Results: Twenty-three studies were eligible with 1418 individual patients in total. Timing of reimaging and clinical reassessment was variable. Absence of recanalization was associated with increased odds of an unfavorable functional outcome (mRS 2-6 versus 0-1; OR, 3.66; 95% CI, 1.73-7.74; p = 0.001), CVT recurrence (OR, 8.81; 95% CI, 1.63-47.7; p = 0.01), and chronic headache (OR, 2.78; 95% CI, 1.16-6.70; p = 0.02). On meta-regression, the relationship between recanalization and mRS differed by the proportion of female patients, where lower proportions of women were associated with higher likelihood of a worse outcome, but not by mean participant age. There was no incremental benefit of full compared with partial recanalization with respect to favorable mRS or recurrence, but odds of chronic headache were higher with partial versus full recanalization (OR, 3.80; 95% CI, 1.43-10.11; p = 0.008). Epilepsy and visual sequelae were not associated with recanalization.
Conclusions: Absence of recanalization was associated with worse functional outcomes, CVT recurrence, and headache, but outcomes were modified by sex. The degree of recanalization was significant in relation to headache outcomes, where partial compared with complete recanalization resulted in a greater likelihood of residual headache. Prospective studies with common timing of repeat clinical-neuroimaging assessments will help to better ascertain the relationship and directionality between the degree of recanalization and outcomes.
Keywords: Modified Rankin Scale; cerebral venous thrombosis; headache; intracranial; meta-analysis; prognosis; recanalization; recurrence; risk factors; sinus thrombosis; thrombosis; venous; vision.
© 2023 The Author(s).
Figures

References
-
- Saposnik G., Barinagarrementeria F., Brown R.D., Jr., Bushnell C.D., Cucchiara B., Cushman M., et al. Diagnosis and management of cerebral venous thrombosis: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2011;42:1158–1192. - PubMed
-
- Ferro J.M., Bousser M.-G., Canhão P., Coutinho J.M., Crassard I., Dentali F., et al. European Stroke Organization guideline for the diagnosis and treatment of cerebral venous thrombosis - endorsed by the European Academy of Neurology. Eur J Neurol. 2017;24:1203–1213. - PubMed
-
- Casais P., Meschengieser S.S., Sanchez-Luceros A., Lazzari M.A. Patients’ perceptions regarding oral anticoagulation therapy and its effect on quality of life. Curr Med Res Opin. 2005;21:1085–1090. - PubMed
-
- Field T.S., Camden M.-C., Al-Shimemeri S., Lui G., Lee A.Y.Y. Antithrombotic strategy in cerebral venous thrombosis: differences between neurologist and hematologist respondents in a Canadian survey. Can J Neurol Sci. 2017;44:116–119. - PubMed
-
- Aguiar de Sousa D., Lucas Neto L., Canhão P., Ferro J.M. Recanalization in cerebral venous thrombosis. Stroke. 2018;49:1828–1835. - PubMed
LinkOut - more resources
Full Text Sources
