

Heterogeneity of treatment effects by risk in pulmonary arterial hypertension
- PMID: 37169384
- PMCID: PMC10919241
- DOI: 10.1183/13993003.00190-2023
Heterogeneity of treatment effects by risk in pulmonary arterial hypertension
Abstract
Background: It is currently unknown if disease severity modifies response to therapy in pulmonary arterial hypertension (PAH). We aimed to explore if disease severity, as defined by established risk-prediction algorithms, modified response to therapy in randomised clinical trials in PAH.
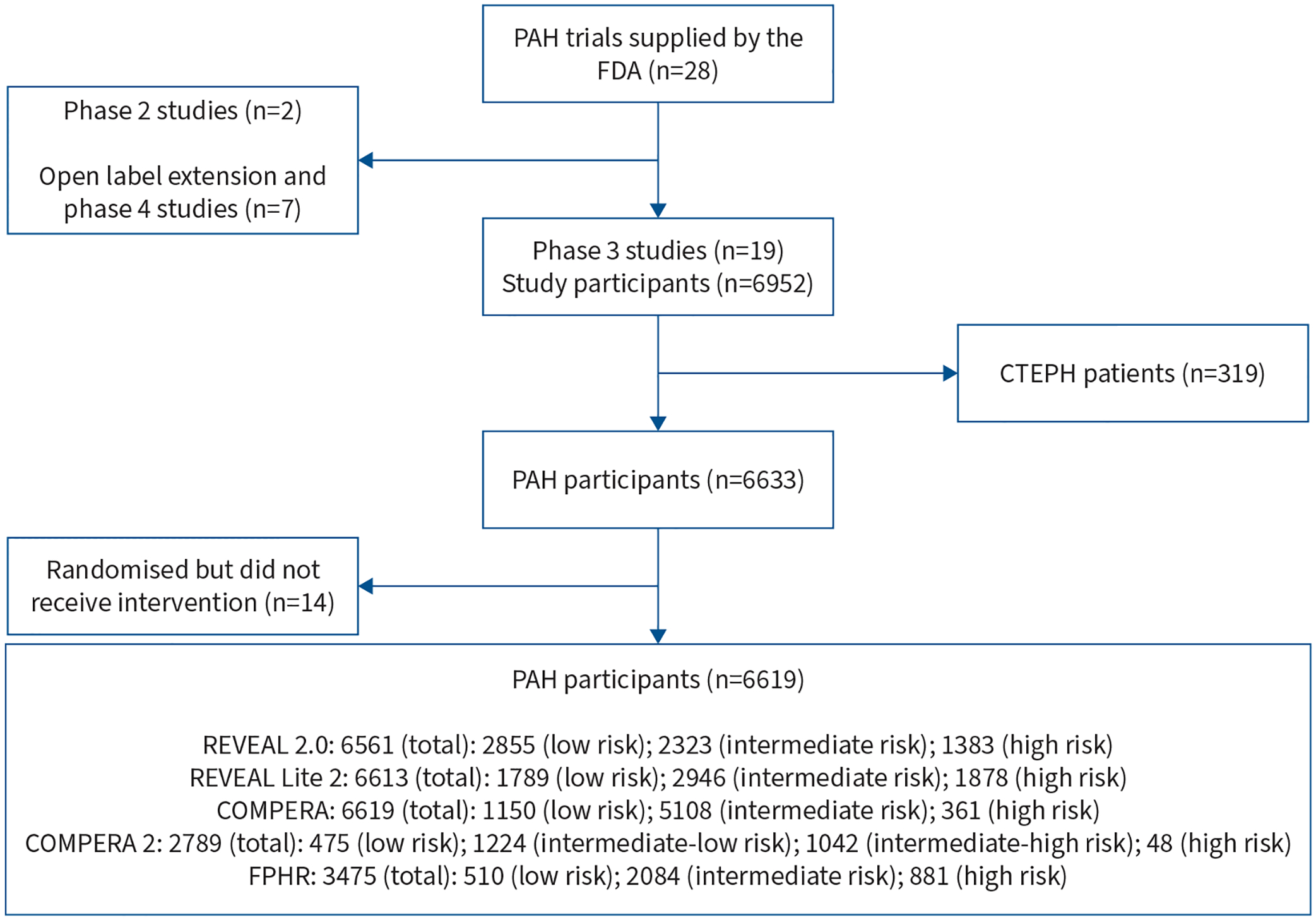
Methods: We performed a meta-analysis using individual participant data from 18 randomised clinical trials of therapy for PAH submitted to the United States Food and Drug Administration to determine if predicted risk of 1-year mortality at randomisation modified the treatment effect on three outcomes: change in 6-min walk distance (6MWD), clinical worsening at 12 weeks and time to clinical worsening.
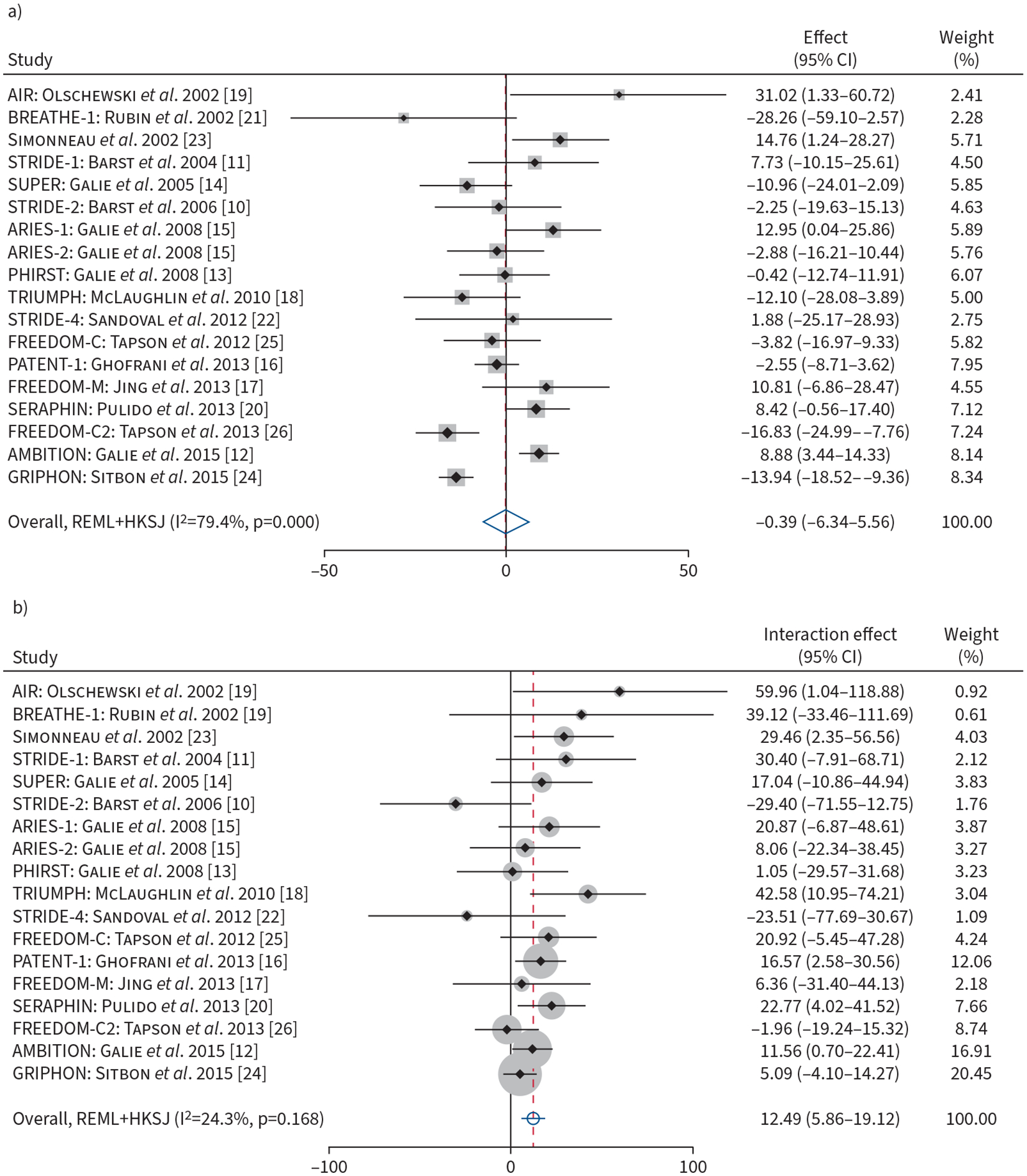
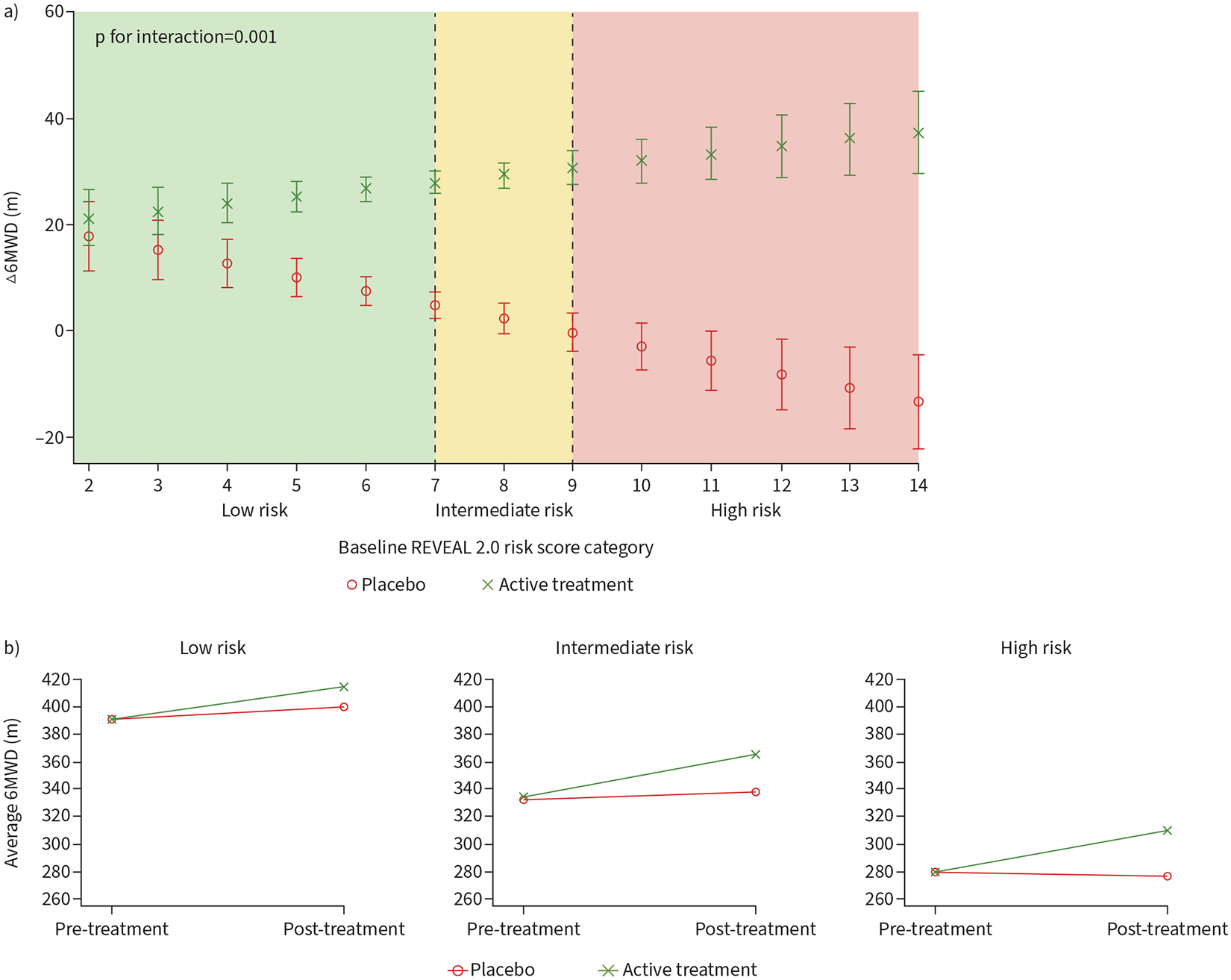
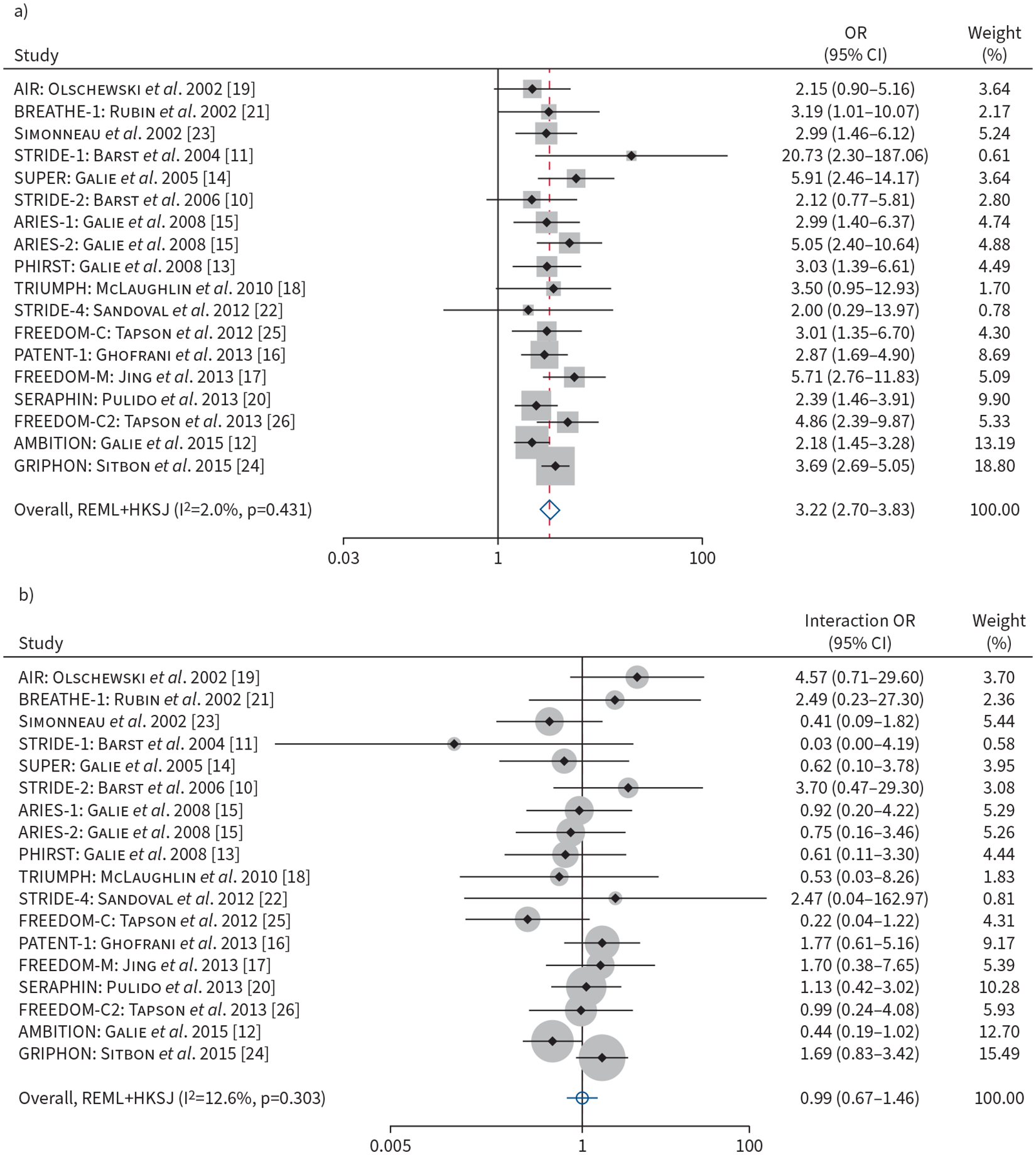
Results: Of 6561 patients with a baseline US Registry to Evaluate Early and Long-Term PAH Disease Management (REVEAL 2.0) score, we found that individuals with higher baseline risk had higher probabilities of clinical worsening but no difference in change in 6MWD. We detected a significant interaction of REVEAL 2.0 risk and treatment assignment on change in 6MWD. For every 3-point increase in REVEAL 2.0 score, there was a 12.49 m (95% CI 5.86-19.12 m; p=0.001) greater treatment effect in change in 6MWD. We did not detect a significant risk by treatment interaction on clinical worsening with most of the risk-prediction algorithms.
Conclusions: We found that predicted risk of 1-year mortality in PAH modified treatment effect as measured by 6MWD, but not clinical worsening. Our findings highlight the importance of identifying sources of treatment heterogeneity by predicted risk to tailor studies to patients most likely to have the greatest treatment response.
Copyright ©The authors 2023. For reproduction rights and permissions contact permissions@ersnet.org.
Conflict of interest statement
Conflict of interest: H-M. Pan has received funding support from the National Institutes of Health (T32HL007891). R.L. McClelland has received full-time-equivalent salary support via a subcontract from the University of Pennsylvania. J.S. Fritz has had grants or contracts from United Therapeutics as monies paid to the institution for the conduct of multicentre pulmonary arterial hypertension drug trials. J.H. Holmes has received funding support from the Cardiovascular Medical Research and Education Fund; has received grants or contracts from the National Institutes of Health, University of Florida Juvenile Diabetes Research Foundation and the University of Pavia; has served as a participant on the Clinical Data to Health External Advisory Board and COACH T2D (Columbia University); and has served unpaid leadership or fiduciary roles for the American College of Medical Informatics, American College of Epidemiology and the Artificial Intelligence Society. J. Minhas has received funding support from the National Institutes of Health (T32HL007891) and the American Thoracic Society Early Career Investigator Award. H.I. Palevsky has participated on a data safety monitoring board for studies for pulmonary arterial hypertension sponsored by United Therapeutics. S.M. Kawut has received funding support from the National Institutes of Health (K24HL103844) and the Cardiovascular Medical Research and Education Fund; received consulting fees from Janssen, Morphic and Regeneron; received payment or honoraria from Janssen; contributed to continuing medical education courses through Accredo, Actelion, Aerovate, Bayer, Inari Medical, Merck, United Therapeutics, Janssen, Liquidia and Pfizer; received support for attending meetings from Aerovate; participated in data safety monitoring boards or advisory boards for United Therapeutics, Acceleron, Vivus and Aerovate; participated in leadership or fiduciary roles for the editorial board of the European Respiratory Journal (ended 2022); received stock or stock options from Verve Therapeutics; and received remote monitory equipment from PhysIQ. N. Al-Naamani has received funding support from the National Institutes of Health (K23HL141584) and from the Cardiovascular Medical Research and Education Fund. The remaining authors disclose no potential conflicts of interest.
Figures
References
-
- McLaughlin VV, Shah SJ, Souza R, et al. Management of pulmonary arterial hypertension. J Am Coll Cardiol 2015; 65: 1976–1997. - PubMed
-
- McLaughlin VV, Archer SL, Badesch DB, et al. ACCF/AHA 2009 expert consensus document on pulmonary hypertension: a report of the American College of Cardiology Foundation Task Force on Expert Consensus Documents and the American Heart Association: developed in collaboration with the American College of Chest Physicians, American Thoracic Society, Inc., and the Pulmonary Hypertension Association. Circulation 2009; 119: 2250–2294. - PubMed
-
- Angus DC, Chang CH. Heterogeneity of treatment effect: estimating how the effects of interventions vary across individuals. JAMA 2021; 326: 2312–2313. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical