

A kidney-brain neural circuit drives progressive kidney damage and heart failure
- PMID: 37169751
- PMCID: PMC10175540
- DOI: 10.1038/s41392-023-01402-x
A kidney-brain neural circuit drives progressive kidney damage and heart failure
Abstract
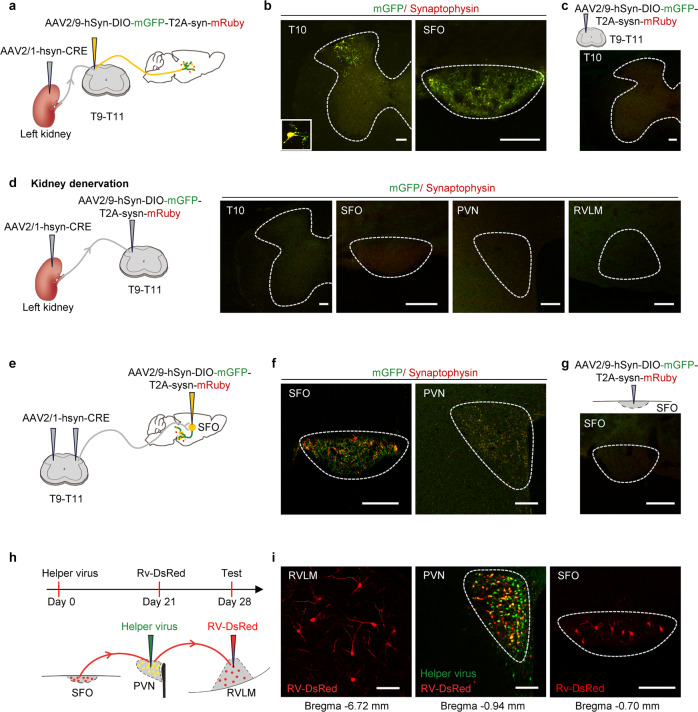
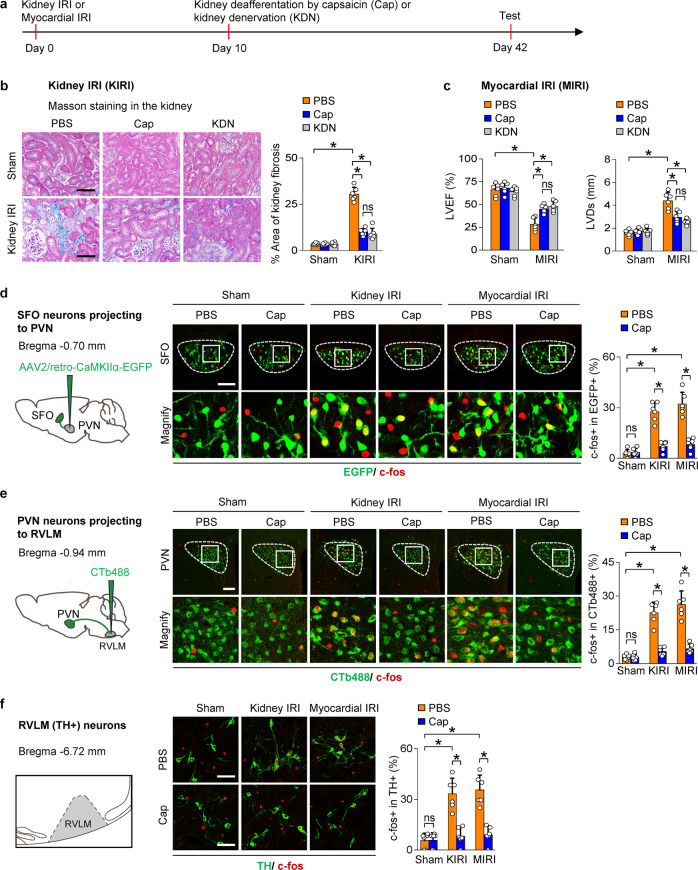
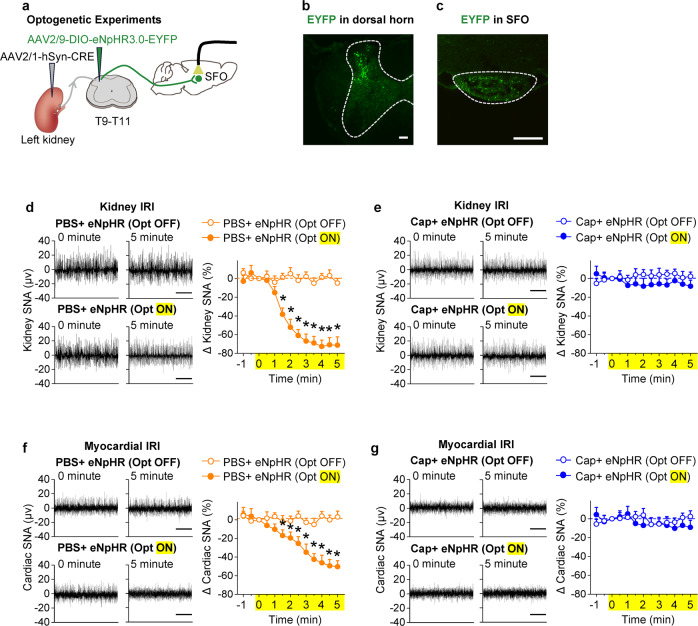
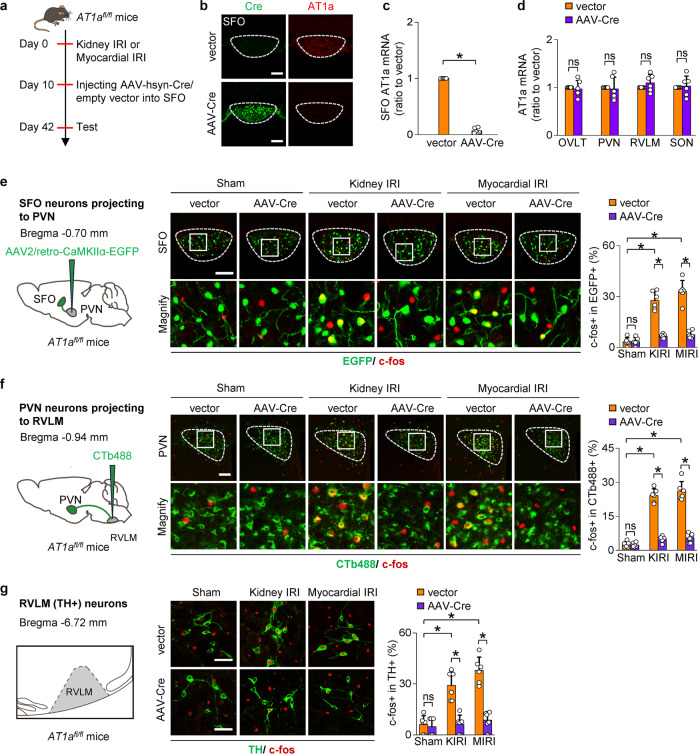
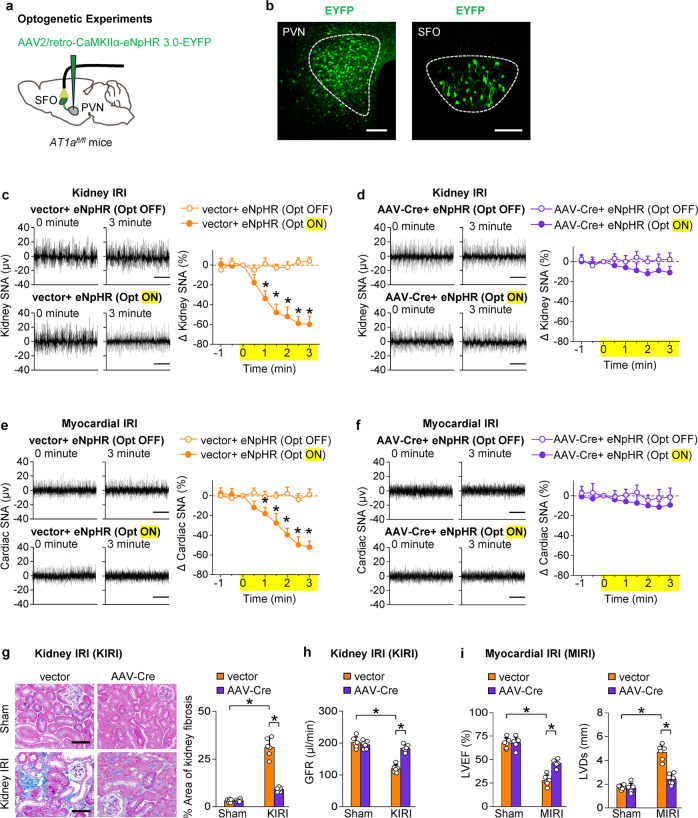
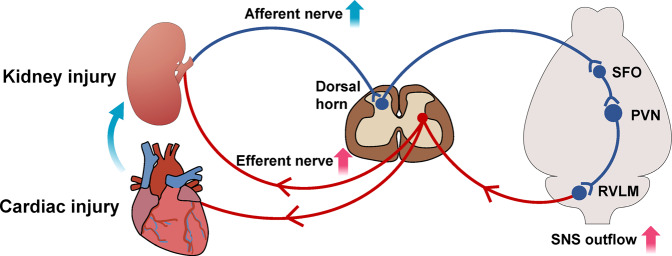
Chronic kidney disease (CKD) and heart failure (HF) are highly prevalent, aggravate each other, and account for substantial mortality. However, the mechanisms underlying cardiorenal interaction and the role of kidney afferent nerves and their precise central pathway remain limited. Here, we combined virus tracing techniques with optogenetic techniques to map a polysynaptic central pathway linking kidney afferent nerves to subfornical organ (SFO) and thereby to paraventricular nucleus (PVN) and rostral ventrolateral medulla that modulates sympathetic outflow. This kidney-brain neural circuit was overactivated in mouse models of CKD or HF and subsequently enhanced the sympathetic discharge to both the kidney and the heart in each model. Interruption of the pathway by kidney deafferentation, selective deletion of angiotensin II type 1a receptor (AT1a) in SFO, or optogenetic silence of the kidney-SFO or SFO-PVN projection decreased the sympathetic discharge and lessened structural damage and dysfunction of both kidney and heart in models of CKD and HF. Thus, kidney afferent nerves activate a kidney-brain neural circuit in CKD and HF that drives the sympathetic nervous system to accelerate disease progression in both organs. These results demonstrate the crucial role of kidney afferent nerves and their central connections in engaging cardiorenal interactions under both physiological and disease conditions. This suggests novel therapies for CKD or HF targeting this kidney-brain neural circuit.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
