

Machine learning for diagnosis of myocardial infarction using cardiac troponin concentrations
- PMID: 37169863
- PMCID: PMC10202804
- DOI: 10.1038/s41591-023-02325-4
Machine learning for diagnosis of myocardial infarction using cardiac troponin concentrations
Abstract
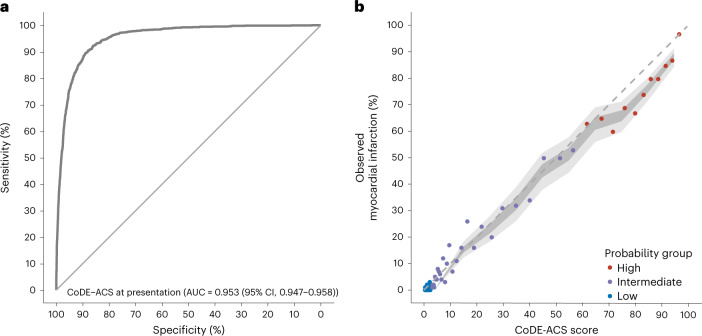
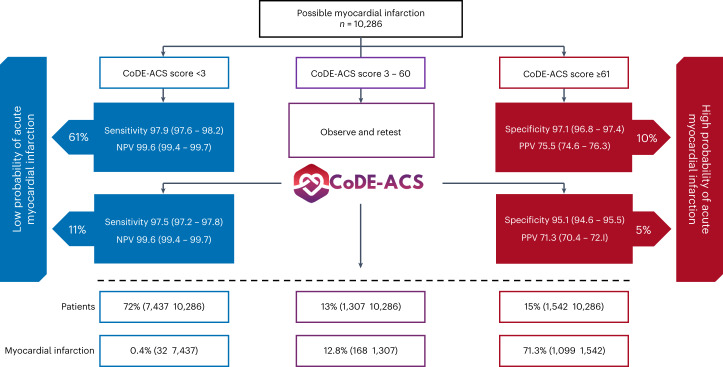
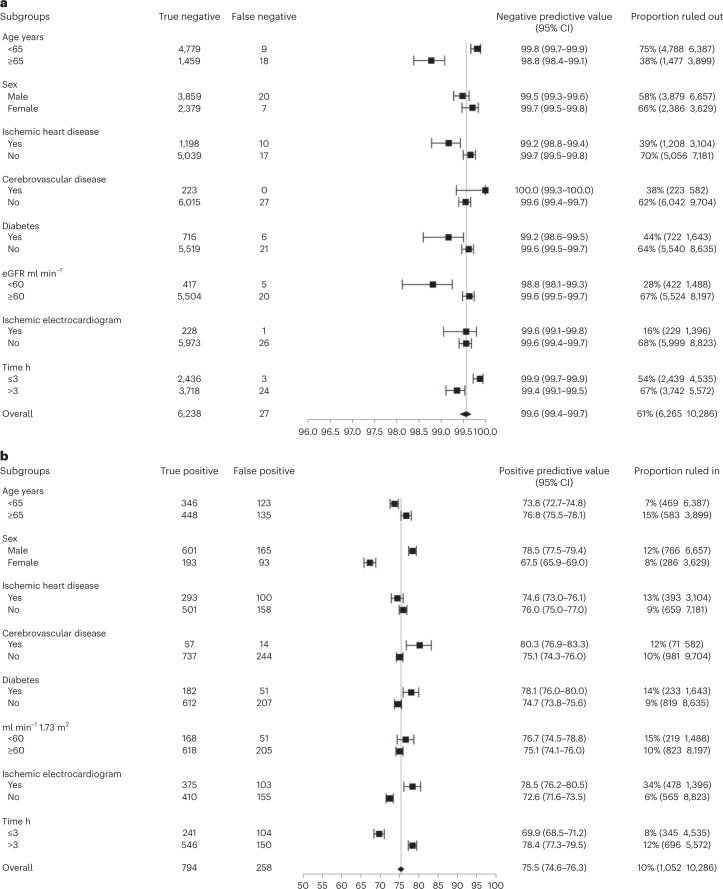
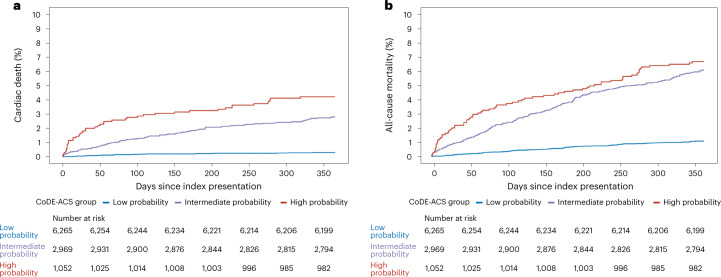
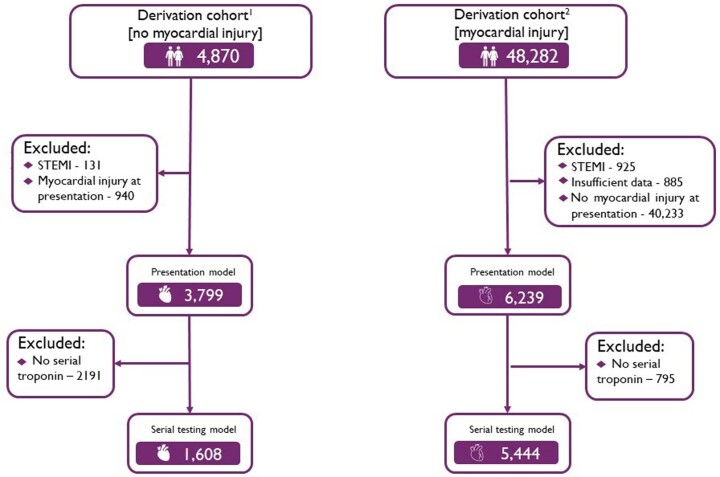
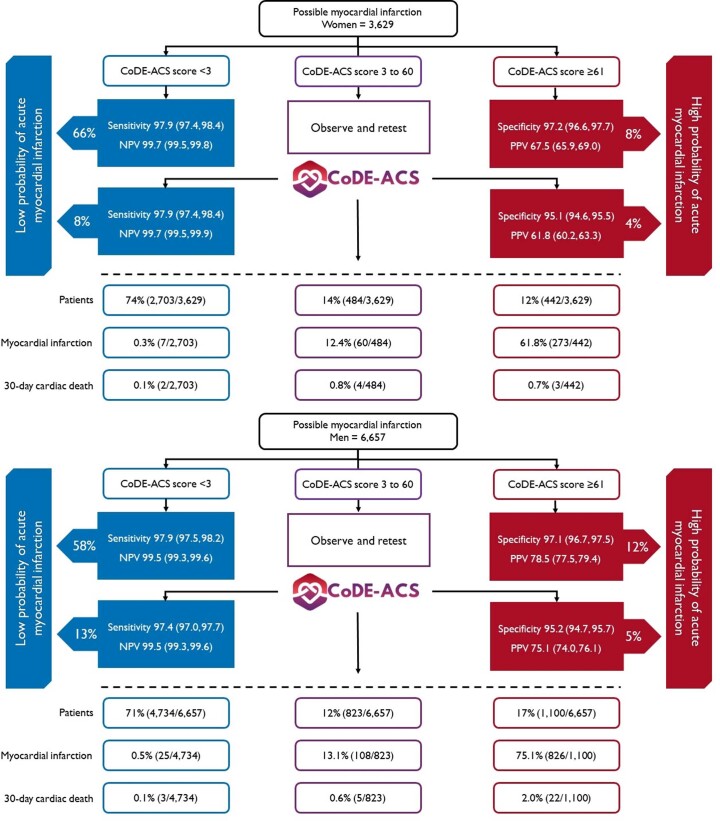
Although guidelines recommend fixed cardiac troponin thresholds for the diagnosis of myocardial infarction, troponin concentrations are influenced by age, sex, comorbidities and time from symptom onset. To improve diagnosis, we developed machine learning models that integrate cardiac troponin concentrations at presentation or on serial testing with clinical features and compute the Collaboration for the Diagnosis and Evaluation of Acute Coronary Syndrome (CoDE-ACS) score (0-100) that corresponds to an individual's probability of myocardial infarction. The models were trained on data from 10,038 patients (48% women), and their performance was externally validated using data from 10,286 patients (35% women) from seven cohorts. CoDE-ACS had excellent discrimination for myocardial infarction (area under curve, 0.953; 95% confidence interval, 0.947-0.958), performed well across subgroups and identified more patients at presentation as low probability of having myocardial infarction than fixed cardiac troponin thresholds (61 versus 27%) with a similar negative predictive value and fewer as high probability of having myocardial infarction (10 versus 16%) with a greater positive predictive value. Patients identified as having a low probability of myocardial infarction had a lower rate of cardiac death than those with intermediate or high probability 30 days (0.1 versus 0.5 and 1.8%) and 1 year (0.3 versus 2.8 and 4.2%; P < 0.001 for both) from patient presentation. CoDE-ACS used as a clinical decision support system has the potential to reduce hospital admissions and have major benefits for patients and health care providers.
© 2023. The Author(s).
Conflict of interest statement
K.K.L. has received honoraria from Abbott Diagnostics. J.B. has received honoraria from Siemens, Roche Diagnostics, Ortho Clinical Diagnostics and Quidel Corporation. P.L.-A. has received speaker’s honoraria or consultancy from Quidel paid to the institution outside the submitted work. L.K. has received honoraria from Roche Diagnostics and Siemens outside the submitted work. F.S.A. has consulted, advised or received honoraria from HyTest Ltd., AWE Medical, Werfen, Siemens Healthineers, Qorvo, Siemens Healthineers and Beckman Coulter. Hennepin Healthcare Research Institute has received research grants from Abbott Diagnostics, Abbott POC, Beckman Dickenson, Beckman Coulter, Ortho Clinical Diagnostics, Roche Diagnostics, Siemens Healthineers and Quidel outside the submitted work. L.C. has received honoraria or consultancy from Abbott Diagnostics, Beckman Coulter and Siemens Healthineers. J.W.P. has undertaken consultancy for Abbott Diagnostics. M.P.T. has received consulting fees or honoraria from Abbott Diagnostics, Roche Diagnostics and Siemens Healthineers; received funding for clinical research from Radiometer; and participated on a Data Safety Monitoring Board/Advisory Board for Abbott Diagnostics, Roche Diagnostics, Siemens Healthineers and Radiometer. C.M. has received research support from Abbott, Beckman Coulter, Brahms, Idorsia, LSI Medience Corporation, Novartis, Ortho Diagnostics, Quidel, Roche, Siemens, Singulex and Sphingotec outside the submitted work as well as speaker honoraria/consulting honoraria from Amgen, Astra Zeneca, Bayer, Boehringer Ingelheim, BMS, Idorsia, Novartis, Osler, Roche and Sanofi all paid to the institution. N.L.M. has received honoraria or consultancy from Abbott Diagnostics, Roche Diagnostics, Siemens Healthineers and LumiraDx. D.D., K.K.L. and N.L.M. are employed by the University of Edinburgh, which has filed a patent on the Collaboration for the Diagnosis and Evaluation of Acute Coronary Syndrome score (patent reference: GB2212464). The remainign authors declare no competing interests. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures









Comment in
-
Machine learning and myocardial infarction diagnosis: sometimes you can't make it on your own.Eur Heart J. 2023 Sep 14;44(35):3309-3310. doi: 10.1093/eurheartj/ehad467. Eur Heart J. 2023. PMID: 37525543 No abstract available.
-
A machine learning-based system to improve myocardial infarction diagnosis.Nat Cardiovasc Res. 2023 Jun;2(6):490. doi: 10.1038/s44161-023-00291-1. Nat Cardiovasc Res. 2023. PMID: 39195884 No abstract available.
References
-
- Than M, et al. A 2-h diagnostic protocol to assess patients with chest pain symptoms in the Asia-Pacific region (ASPECT): a prospective observational validation study. Lancet. 2011;377:1077–1084. - PubMed
-
- Body R, et al. Rapid exclusion of acute myocardial infarction in patients with undetectable troponin using a high-sensitivity assay. J. Am. Coll. Cardiol. 2011;58:1332–1339. - PubMed
-
- Reichlin T, et al. One-hour rule-out and rule-in of acute myocardial infarction using high-sensitivity cardiac troponin T. Arch. Intern. Med. 2012;172:1211–1218. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
