

COVID-19 vaccine hesitancy and social contact patterns in Pakistan: results from a national cross-sectional survey
- PMID: 37170085
- PMCID: PMC10174611
- DOI: 10.1186/s12879-023-08305-w
COVID-19 vaccine hesitancy and social contact patterns in Pakistan: results from a national cross-sectional survey
Abstract
Background: Vaccination is a key tool against COVID-19. However, in many settings it is not clear how acceptable COVID-19 vaccination is among the general population, or how hesitancy correlates with risk of disease acquisition. In this study we conducted a nationally representative survey in Pakistan to measure vaccination perceptions and social contacts in the context of COVID-19 control measures and vaccination programmes.
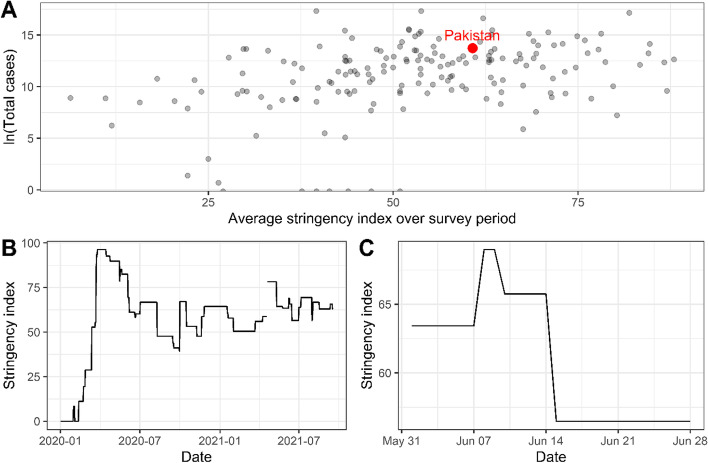
Methods: We conducted a vaccine perception and social contact survey with 3,658 respondents across five provinces in Pakistan, between 31 May and 29 June 2021. Respondents were asked a series of vaccine perceptions questions, to report all direct physical and non-physical contacts made the previous day, and a number of other questions regarding the social and economic impact of COVID-19 and control measures. We examined variation in perceptions and contact patterns by geographic and demographic factors. We describe knowledge, experiences and perceived risks of COVID-19. We explored variation in contact patterns by individual characteristics and vaccine hesitancy, and compared to patterns from non-pandemic periods.
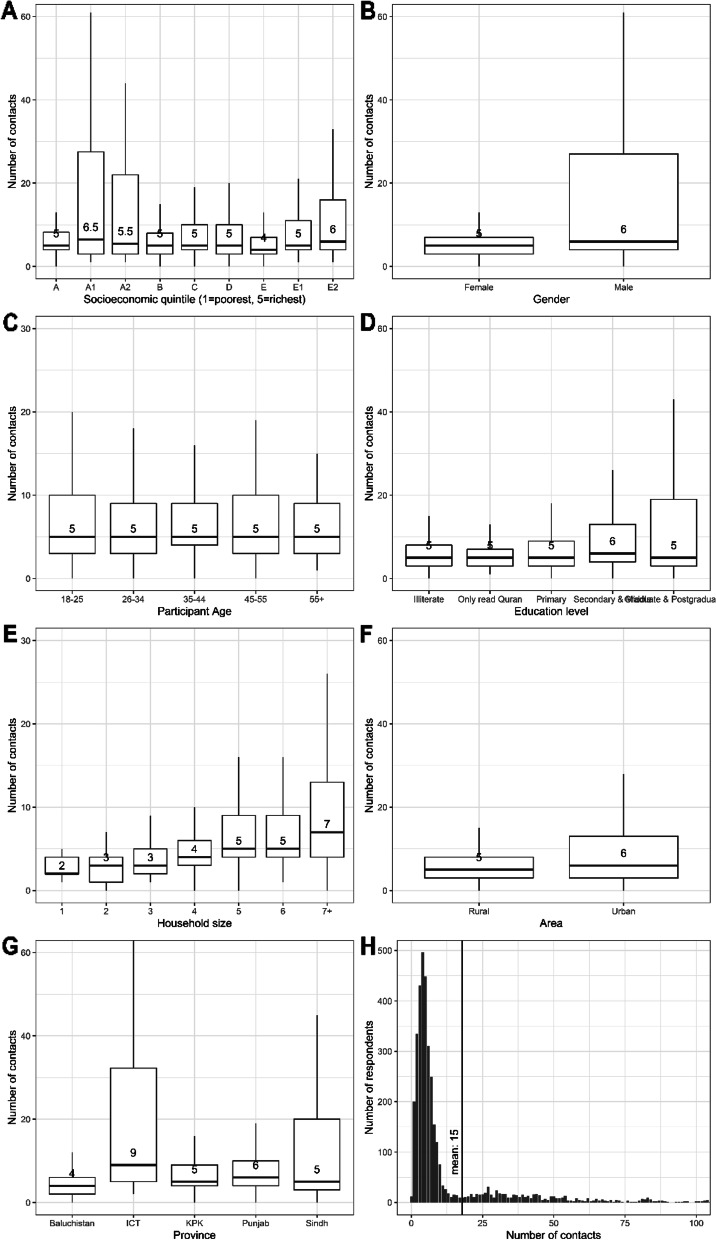
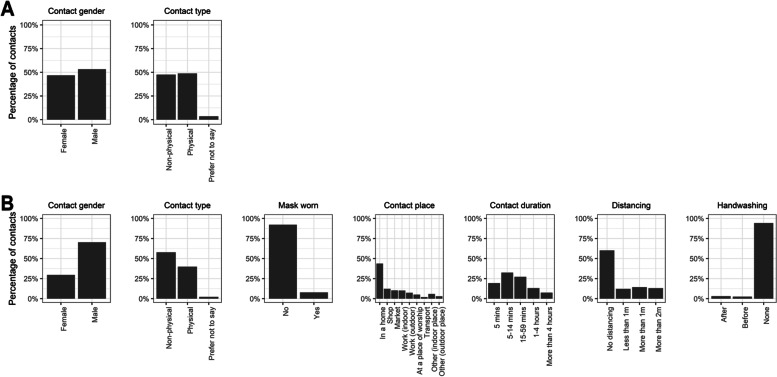
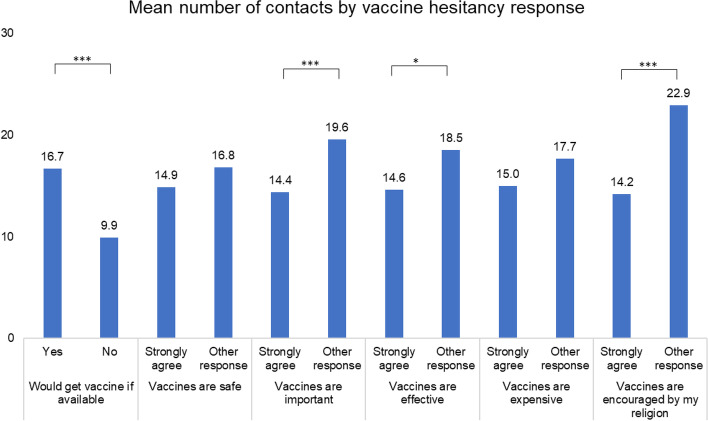
Results: Self-reported adherence to self-isolation guidelines was poor, and 51% of respondents did not know where to access a COVID-19 test. Although 48.1% of participants agreed that they would get a vaccine if offered, vaccine hesitancy was higher than in previous surveys, and greatest in Sindh and Baluchistan provinces and among respondents of lower socioeconomic status. Participants reported a median of 5 contacts the previous day (IQR: 3-5, mean 14.0, 95%CI: 13.2, 14.9). There were no substantial differences in the number of contacts reported by individual characteristics, but contacts varied substantially among respondents reporting more or less vaccine hesitancy. Contacts were highly assortative, particularly outside the household where 97% of men's contacts were with other men. We estimate that social contacts were 9% lower than before the COVID-19 pandemic.
Conclusions: Although the perceived risk of COVID-19 in Pakistan is low in the general population, around half of participants in this survey indicated they would get vaccinated if offered. Vaccine impact studies which do not account for correlation between social contacts and vaccine hesitancy may incorrectly estimate the impact of vaccines, for example, if unvaccinated people have more contacts.
Keywords: COVID-19; Physical distancing; SARS-CoV2; Social contacts; Vaccine perceptions.
© 2023. The Author(s).
Conflict of interest statement
Since initial submission of this work MQ moved to a full-time position at Evidera, a commercial pharmaceutical consultancy; he does not work on products related to the content of this manuscript. All other authors declare no competing interest.
Figures

References
-
- Ministry of National Health Services Regulation and Coordination. Service Statistics. 2022; Available from: https://ncoc.gov.pk/covid-vaccination-en.php.
-
- Cabore JW, Karamagi HC, Kipruto H, Asamani JA, Droti B, Seydi ABW, Titi-Ofei R, Impouma B, Yao M, Yoti Z, Zawaira F, Tumusiime P, Talisuna A, Kasolo FC, Moeti MR. The potential effects of widespread community transmission of SARS-CoV-2 infection in the World Health Organization African Region: a predictive model. BMJ Glob Health. 2020;5(5):e002647. - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
