

Novel external reinforcement device for gastrointestinal anastomosis in an experimental study
- PMID: 37170107
- PMCID: PMC10176862
- DOI: 10.1186/s12893-023-02027-1
Novel external reinforcement device for gastrointestinal anastomosis in an experimental study
Abstract
Background: Anastomotic leakage has been reported to occur when the load on the anastomotic site exceeds the resistance created by sutures, staples, and early scars. It may be possible to avoid anastomotic leakage by covering and reinforcing the anastomotic site with a biocompatible material. The aim of this study was to evaluate the safety and feasibility of a novel external reinforcement device for gastrointestinal anastomosis in an experimental model.
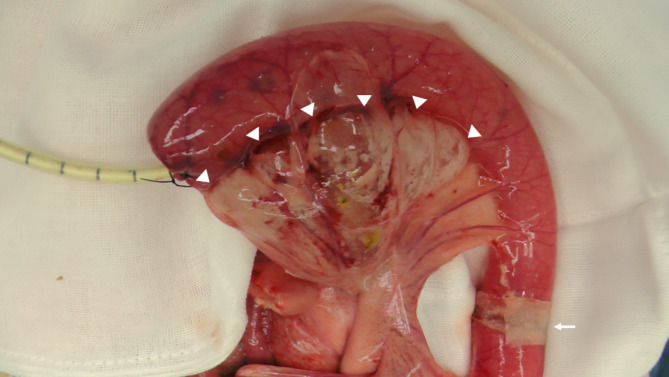
Methods: A single pig was used in this non-survival study, and end-to-end anastomoses were created in six small bowel loops by a single-stapling technique using a circular stapler. Three of the six anastomoses were covered with a novel external reinforcement device. Air was injected, a pressure test of each anastomosis was performed, and the bursting pressure was measured.
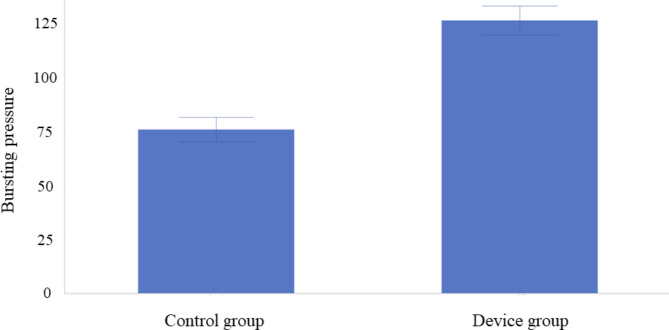
Results: Reinforcement of the anastomotic site with the device was successfully performed in all anastomoses. The bursting pressure was 76.1 ± 5.7 mmHg in the control group, and 126.8 ± 6.8 mmHg in the device group, respectively. The bursting pressure in the device group was significantly higher than that in the control group (p = 0.0006).
Conclusions: The novel external reinforcement device was safe and feasible for reinforcing the anastomoses in the experimental model.
Keywords: Anastomosis; Anastomotic leakage; Colorectal surgery; Reinforcement; Sealant.
© 2023. The Author(s).
Conflict of interest statement
HH, NT, and MI received experimental animals and a novel external reinforcement device for gastrointestinal anastomosis from BMG Incorporated, Kyoto, Japan. National cancer center, WH and SHH have a patent of the novel external reinforcement device. WH and SHH are employees of BMG Incorporated, Kyoto, Japan. WH and SHH had no role in the analysis or interpretation of the data. Conflicts of interest are properly managed in accordance with the regulations of each institution.
Figures





References
-
- Snijders HS, Wouters MW, van Leersum NJ, Kolfschoten NE, Henneman D, de Vries AC, et al. Meta-analysis of the risk for anastomotic leakage, the postoperative mortality caused by leakage in relation to the overall postoperative mortality. Eur J Surg Oncol. 2012;38:1013–9. doi: 10.1016/j.ejso.2012.07.111. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
