

Dose and time-response effect of photobiomodulation therapy on glycemic control in type 2 diabetic patients combined or not with hypoglycemic medicine: A randomized, crossover, double-blind, sham-controlled trial
- PMID: 37171054
- PMCID: PMC10662441
- DOI: 10.1002/jbio.202300083
Dose and time-response effect of photobiomodulation therapy on glycemic control in type 2 diabetic patients combined or not with hypoglycemic medicine: A randomized, crossover, double-blind, sham-controlled trial
Abstract
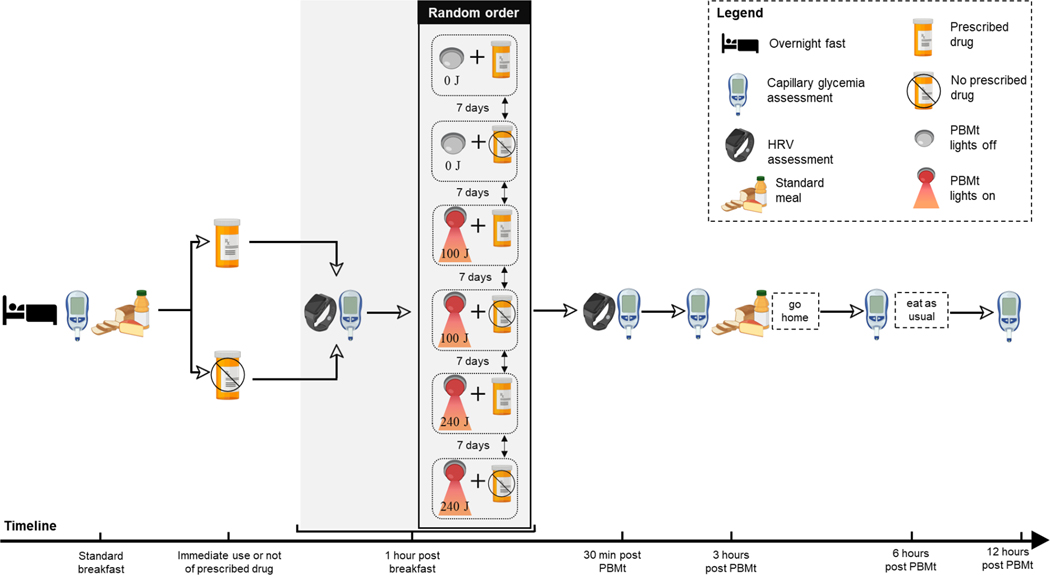
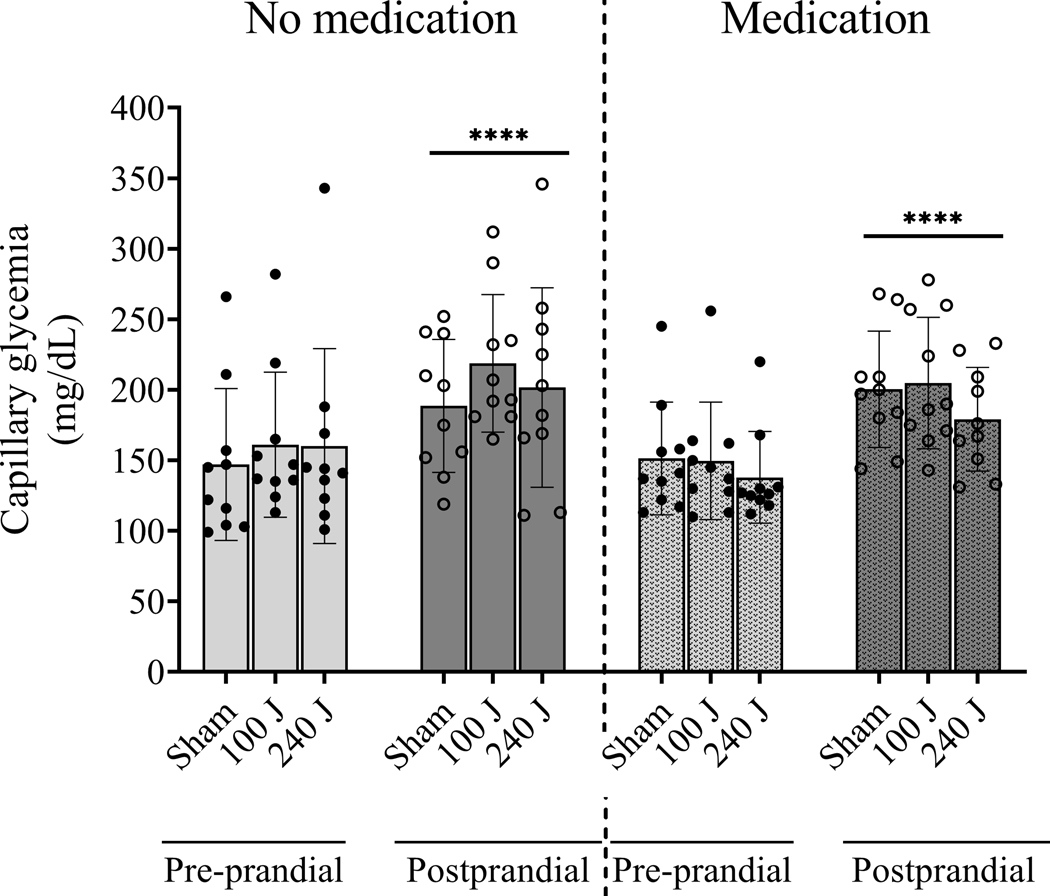
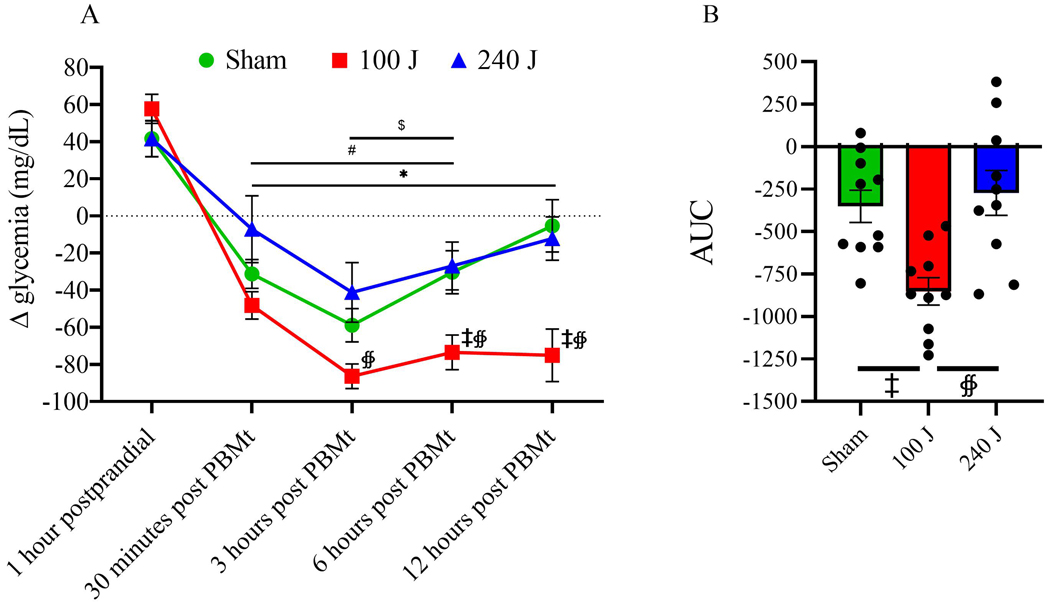
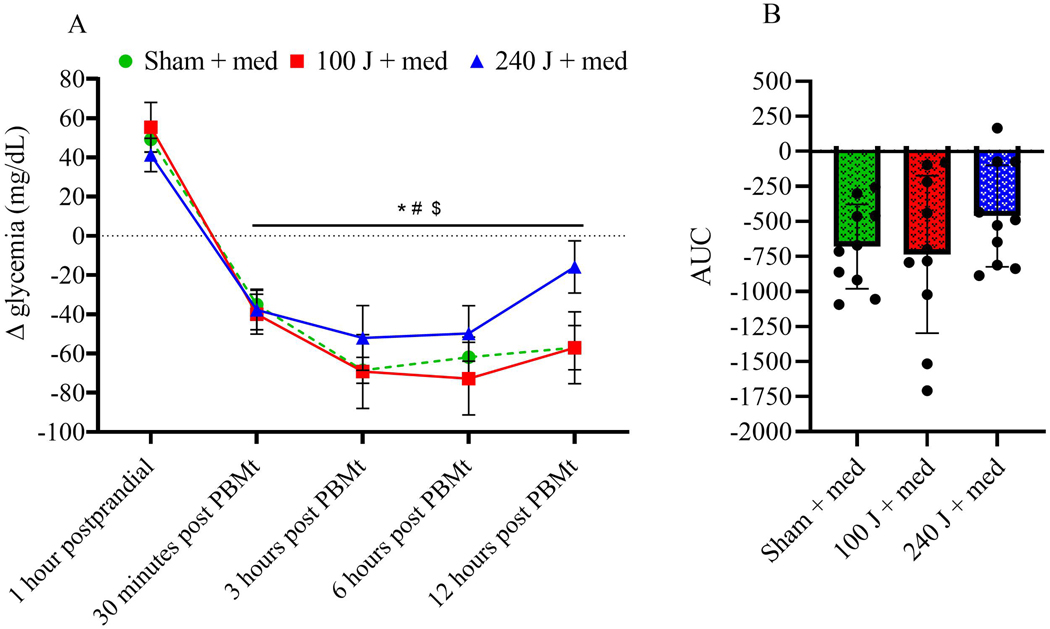
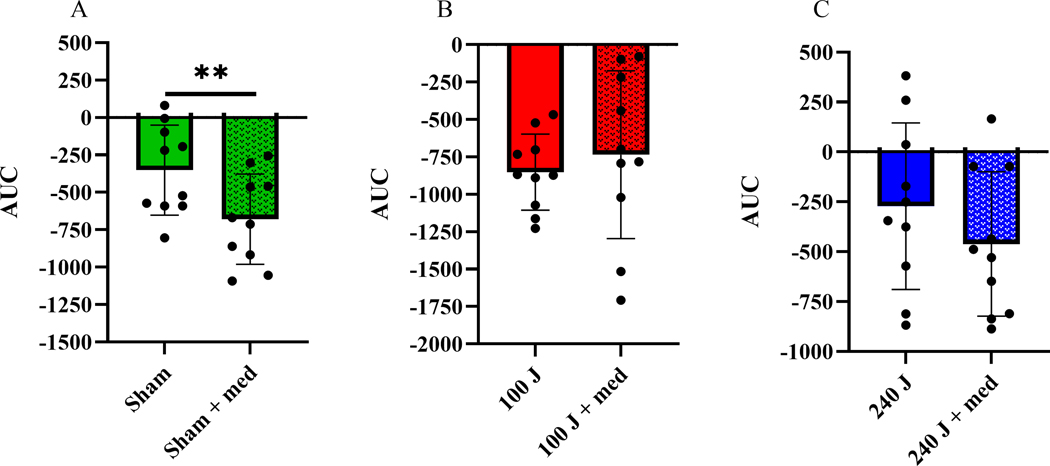
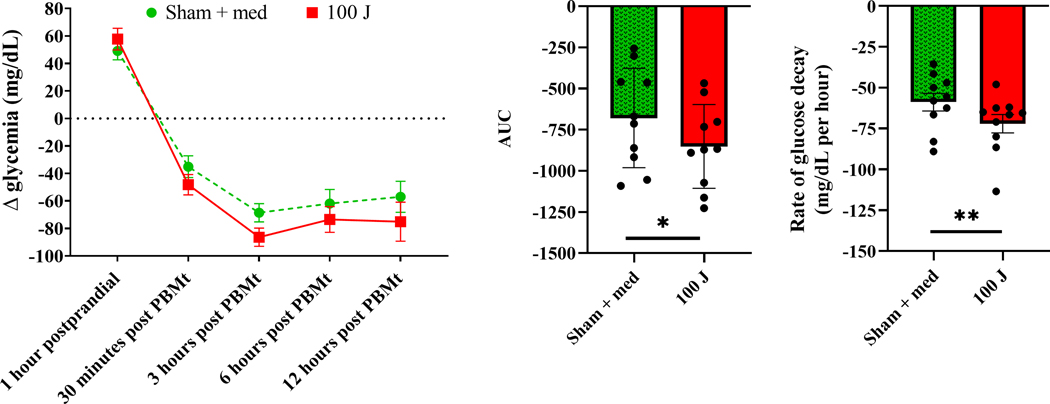
Photobiomodulation therapy (PBMt) combined or not with oral hypoglycemic medication has not been investigated in type 2 diabetes (T2DM) patients. All 10 T2DM patients were assessed randomly at 6 different occasions (3 with and 3 without regular oral hypoglycemic medication). Capillary glycemia was assessed after overnight fast (pre-prandial), 1 h postprandially (standardized meal, 338 kcal), and 30 min, 3 h, 6 h, 12 h post-PBMt (830 nm; 25 arrays of LEDs, 80 mW/array). Three doses (0 J-sham, 100 J, 240 J per site) were applied bilaterally on quadriceps femoris muscles, hamstrings, triceps surae, ventral upper arm and forearm; and randomly combined or not with oral hypoglicemic medication, totaling six different therapies applied for all 10 TDM2 patients (PBMt sham, PBMt 100 J, PBMt 240 J, PBMt sham + medication, PBMt 100 J + medication, PBMt 240 J + medication). Cardiac autonomic control was assessed by heart rate variability (HRV) indices. Without medication, there was reduction in glycemia after all PBMt doses, with 100 J as the best dose that persisted until 12 h and presented lower area under the curve (AUC). With medication, glycemia decreased similarly among doses. No differences between 100 J and sham + medication, but AUC was significantly lower after 100 J, suggesting better glycemic control. Low frequency component of HRV increased after sham + medication and 100 J, suggesting higher sympathetic activation. PBMt showed time- and dose-response effect to reduce glycemia in T2DM patients. Effects on HRV were consistent with glycemic control.
Keywords: dose-response; glycemic control; heart rate variability; hypoglycemic drugs; insulin resistance; photobiomodulation therapy.
© 2023 Wiley-VCH GmbH.
Conflict of interest statement
CONFLICT OF INTEREST
MRH declares the following potential conflicts of interest. Scientific Advisory Boards: Transdermal Cap Inc, Cleveland, OH; Hologenix Inc. Santa Monica, CA; Vielight, Toronto, Canada; JOOVV Inc, Minneapolis-St. Paul MN; Sunlighten, Kansas City, MO; Consulting; USHIO Corp, Japan; Sanofi-Aventis Deutschland GmbH, Frankfurt am Main, Germany; Klox Asia, Guangzhou, China. Stockholding: Niraxx Light Therapeutics, Inc, Irvine CA; JelikaLite Corp, New York NY. The other authors declare no conflict of interest.
Figures

Similar articles
-
Can photobiomodulation therapy (PBMT) control blood glucose levels and alter muscle glycogen synthesis?J Photochem Photobiol B. 2020 Jun;207:111877. doi: 10.1016/j.jphotobiol.2020.111877. Epub 2020 Apr 7. J Photochem Photobiol B. 2020. PMID: 32298941
-
Dose-response effect of photobiomodulation therapy on neuromuscular economy during submaximal running.Lasers Med Sci. 2018 Feb;33(2):329-336. doi: 10.1007/s10103-017-2378-4. Epub 2017 Nov 3. Lasers Med Sci. 2018. PMID: 29101708 Clinical Trial.
-
Time-Response of Photobiomodulation Therapy by Light-Emitting Diodes on Muscle Torque and Fatigue Resistance in Young Men: Randomized, Double-Blind, Crossover and Placebo-Controlled Study.Photobiomodul Photomed Laser Surg. 2020 Dec;38(12):750-757. doi: 10.1089/photob.2020.4813. Epub 2020 Nov 23. Photobiomodul Photomed Laser Surg. 2020. PMID: 33227220 Clinical Trial.
-
Photobiomodulation Therapy on the Treatment of Insulin Resistance: A Narrative Review.Photobiomodul Photomed Laser Surg. 2022 Sep;40(9):597-603. doi: 10.1089/photob.2022.0031. Epub 2022 Aug 30. Photobiomodul Photomed Laser Surg. 2022. PMID: 36040371 Review.
-
Photobiomodulation therapy (PBMT) in skeletal muscle regeneration: A comprehensive review of mechanisms, clinical applications, and future directions.Photodiagnosis Photodyn Ther. 2025 Jun;53:104634. doi: 10.1016/j.pdpdt.2025.104634. Epub 2025 May 15. Photodiagnosis Photodyn Ther. 2025. PMID: 40381876 Review.
Cited by
-
Long-term safety of photobiomodulation exposure to beta cell line and rat islets in vitro and in vivo.Sci Rep. 2024 Nov 6;14(1):26874. doi: 10.1038/s41598-024-77660-8. Sci Rep. 2024. PMID: 39505966 Free PMC article.
-
Photobiomodulation for diabetes and its complications: a review of general presentation, mechanisms and efficacy.Ann Med. 2024 Dec;56(1):2433684. doi: 10.1080/07853890.2024.2433684. Epub 2024 Nov 28. Ann Med. 2024. PMID: 39607829 Free PMC article. Review.
-
Photobiomodulation therapy (red/NIR LEDs) reduced the length of stay in intensive care unit and improved muscle function: A randomized, triple-blind, and sham-controlled trial.J Biophotonics. 2024 May;17(5):e202300501. doi: 10.1002/jbio.202300501. Epub 2024 Jan 23. J Biophotonics. 2024. PMID: 38262071 Free PMC article. Clinical Trial.
-
The dose-effect response of combined red and infrared photobiomodulation on insulin resistance in skeletal muscle cells.Biochem Biophys Rep. 2024 Sep 26;40:101831. doi: 10.1016/j.bbrep.2024.101831. eCollection 2024 Dec. Biochem Biophys Rep. 2024. PMID: 39398538 Free PMC article.
-
Diabetes in spotlight: current knowledge and perspectives of photobiomodulation utilization.Front Endocrinol (Lausanne). 2024 Mar 19;15:1303638. doi: 10.3389/fendo.2024.1303638. eCollection 2024. Front Endocrinol (Lausanne). 2024. PMID: 38567306 Free PMC article. Review.
References
-
- DeFronzo RA, Ferrannini E, Groop L, Henry RR, Herman WH, Holst JJ, Hu FB, Kahn CR, Raz I, Shulman GI, Simonson DC, Testa MA, Weiss R. Nature reviews. Disease primers. 2015, 1, 15019. - PubMed
-
- Fowler MJ Clinical Diabetes. 2008, 26, 77–82.
-
- Saeedi P, Petersohn I, Salpea P, Malanda B, Karuranga S, Unwin N, Colagiuri S, Guariguata L, Motala AA, Ogurtsova K, Shaw JE, Bright D, Williams R. Diabetes Research and Clinical Practice. 2019, 157, 107843. - PubMed
-
- Karayannis G, Giamouzis G, Cokkinos DV, Skoularigis J, Triposkiadis F. Expert review of cardiovascular therapy. 2012, 10, 747–765. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
