

High-grade B-cell lymphoma, not otherwise specified: a multi-institutional retrospective study
- PMID: 37171397
- PMCID: PMC10598493
- DOI: 10.1182/bloodadvances.2023009731
High-grade B-cell lymphoma, not otherwise specified: a multi-institutional retrospective study
Abstract
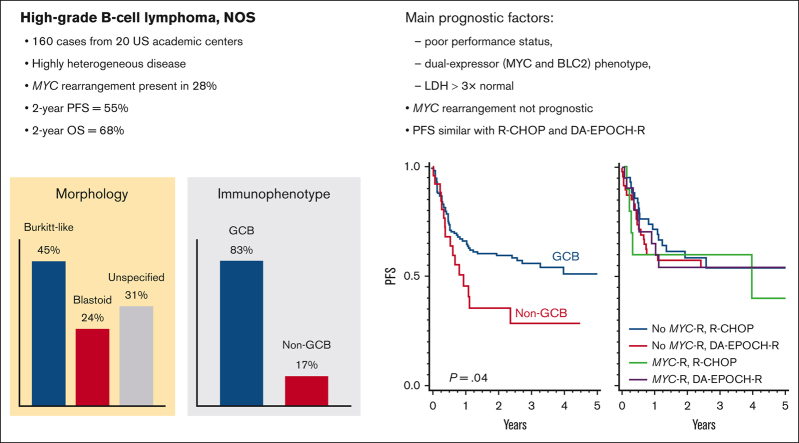
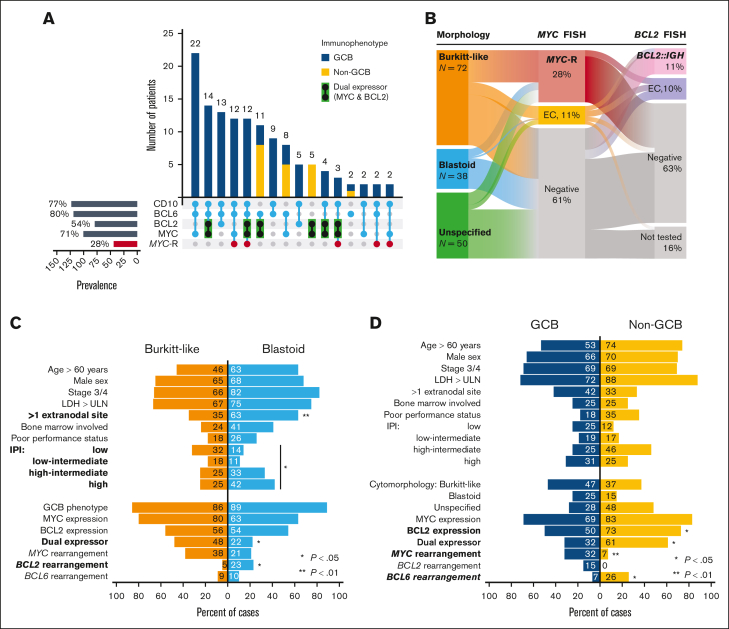
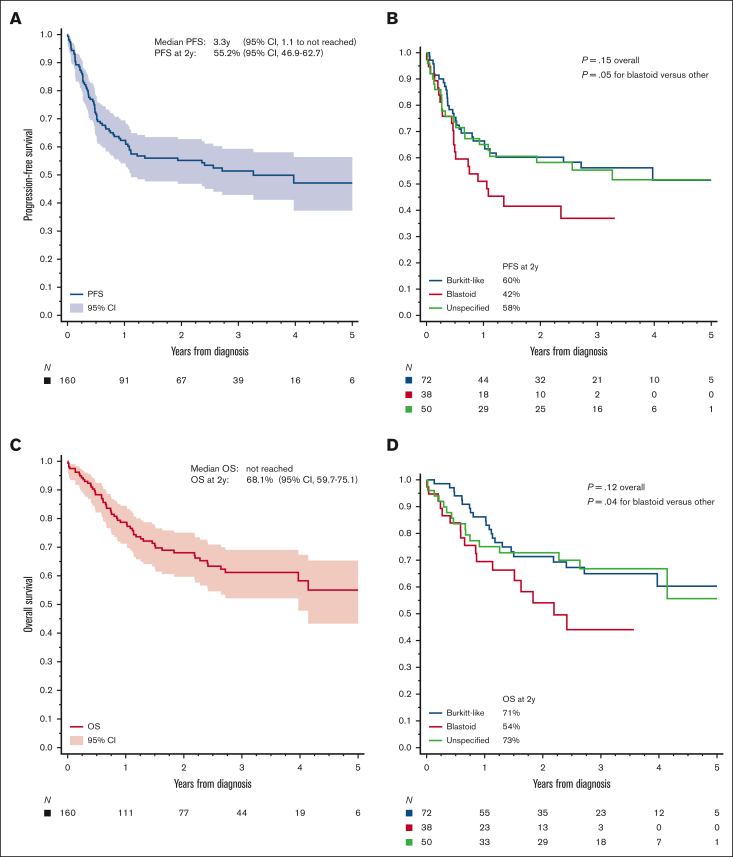
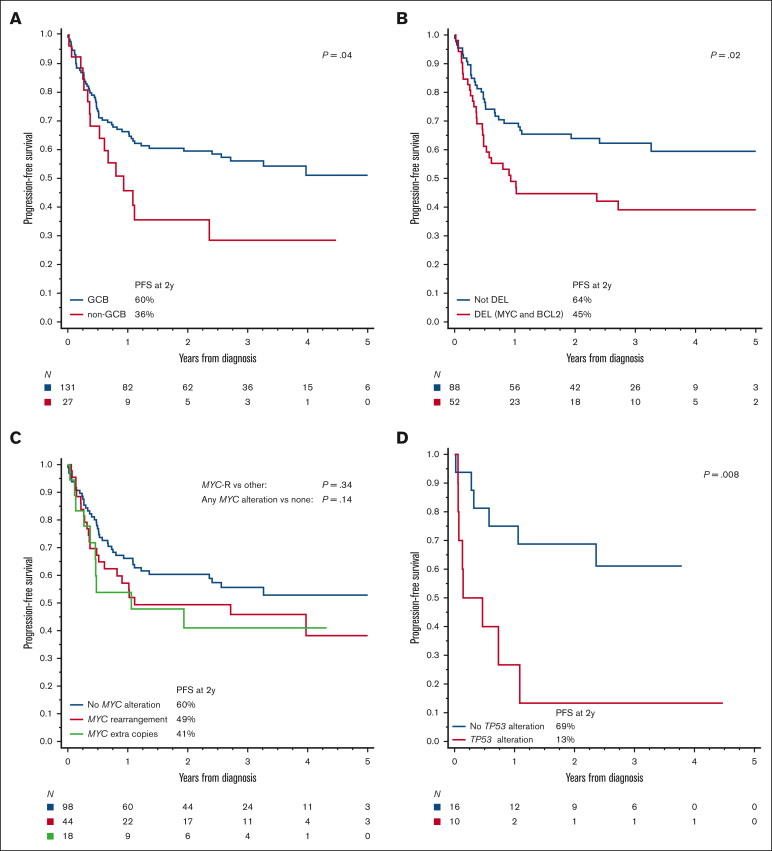
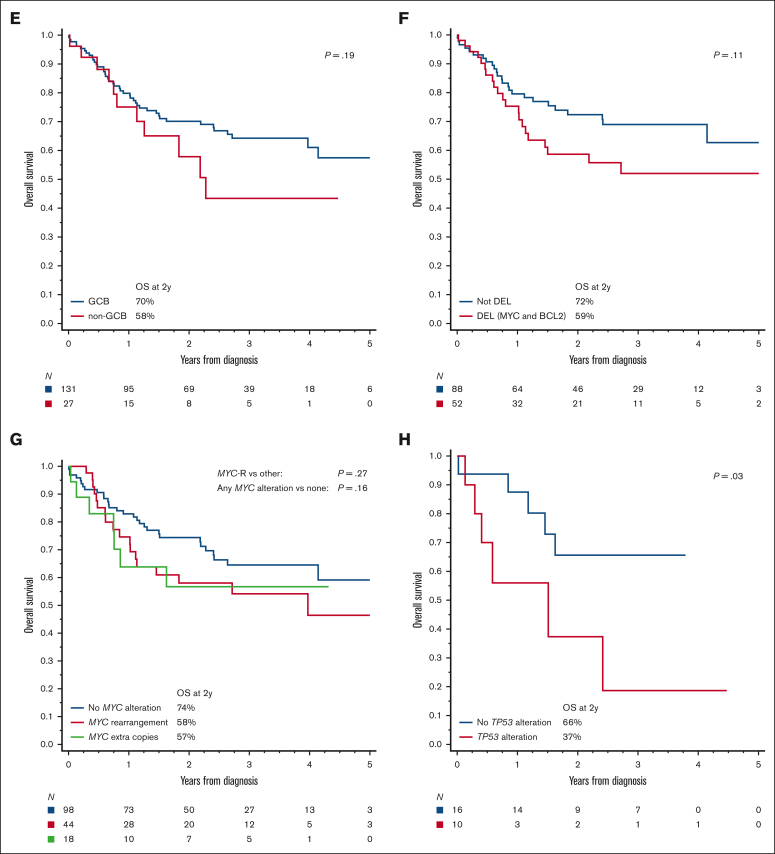
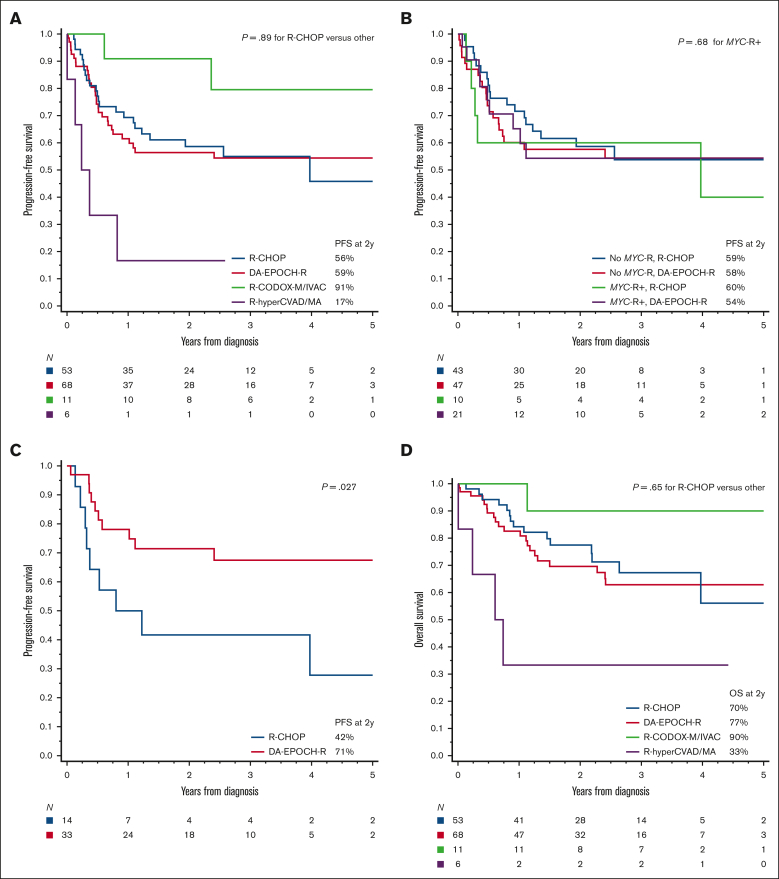
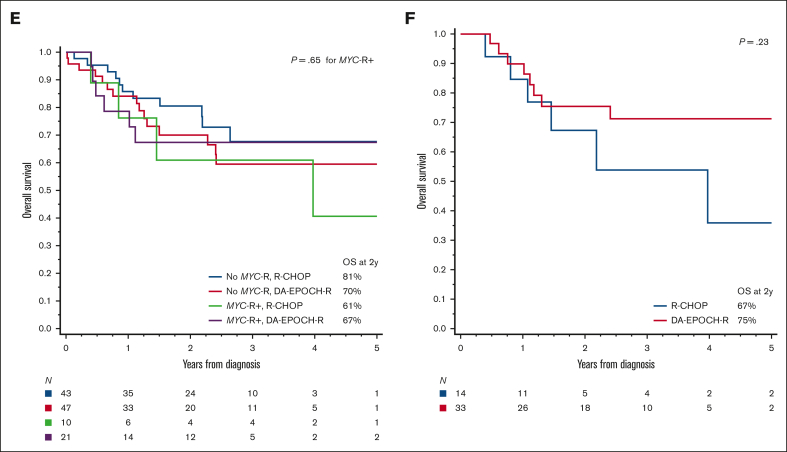
In this multi-institutional retrospective study, we examined the characteristics and outcomes of 160 patients with high-grade B-cell lymphoma, not otherwise specified (HGBL-NOS)-a rare category defined by high-grade morphologic features and lack of MYC rearrangements with BCL2 and/or BCL6 rearrangements ("double hit"). Our results show that HGBL-NOS tumors are heterogeneous: 83% of patients had a germinal center B-cell immunophenotype, 37% a dual-expressor immunophenotype (MYC and BCL2 expression), 28% MYC rearrangement, 13% BCL2 rearrangement, and 11% BCL6 rearrangement. Most patients presented with stage IV disease, a high serum lactate dehydrogenase, and other high-risk clinical factors. Most frequent first-line regimens included dose-adjusted cyclophosphamide, doxorubicin, vincristine, and etoposide, with rituximab and prednisone (DA-EPOCH-R; 43%); rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP; 33%); or other intensive chemotherapy programs. We found no significant differences in the rates of complete response (CR), progression-free survival (PFS), or overall survival (OS) between these chemotherapy regimens. CR was attained by 69% of patients. PFS at 2 years was 55.2% and OS was 68.1%. In a multivariable model, the main prognostic factors for PFS and OS were poor performance status, lactate dehydrogenase >3 × upper limit of normal, and a dual-expressor immunophenotype. Age >60 years or presence of MYC rearrangement were not prognostic, but patients with TP53 alterations had a dismal PFS. Presence of MYC rearrangement was not predictive of better PFS in patients treated with DA-EPOCH-R vs R-CHOP. Improvements in the diagnostic criteria and therapeutic approaches beyond dose-intense chemotherapy are needed to overcome the unfavorable prognosis of patients with HGBL-NOS.
© 2023 by The American Society of Hematology. Licensed under Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0), permitting only noncommercial, nonderivative use with attribution. All other rights reserved.
Conflict of interest statement
Conflict-of-interest disclosure: N.E. reports financial support from Pharmacyclics, Seattle Genetics, BeiGene, TG Therapeutics, Novartis, and Incyte. D.J.L. reports financial support from MorphoSys, Calithera, Karyopharm, Epizyme, Curis Inc, ADC Therapeutics, and Triphase. M.E.H. reports financial support from AbbVie, Acerta Pharma, AstraZeneca, Genzyme, and Karyopharm. G.S.N. NanoString, Roche, TG Therapeutics, Zai Lab, Bristol Myers Squibb (BMS)/Celgene, Selvita, Ryvu Therapeutics, MorphoSys US Inc, Kymera Therapeutics, Kite Pharma Inc, Karyopharm, Incyte, Genentech Inc, F. Hoffmann-La Roche Ltd, Daiichi Sankyo Inc, Curis Inc, Celgene Corporation/BMS, Blueprint Medicines Corporation, and Bantam Pharmaceutical. J.S.-S. served on the speaker’s bureu for Seagen and consulted for (advisory boards) TG Therapeutics, AbbVie, ADC therapeutics, Janssen, MorphoSys/Incyte, and MassiveBio. S.K.K. reports financial support from Radyus Research, Karyopharm, and Incyte Pharmaceuticals. M.L.X. reports financial support from Pure Marrow and Blueprint Medicines. P.T. reports financial support from TG Therapeutics, Genentech, ADC Therapeutics, Epizyme, Targeted Oncology, Physician Education Review, and Lilly USA. S.D.S. reports financial support from Portola Pharmaceuticals, Numab Therapeutics AG, Nanjing Pharmaceuticals Co Ltd, MorphoSys, Merck Sharp/Dohme Corp, Kymera Therapeutics, KITE pharma, Karyopharm, Incyte Corporation, Genentech, Epizyme, Enterome, Denovo Biopharma, BeiGene, Bayer, AstraZeneca, ADC Therapeutics, AbbVie, and Viracta Therapeutics. D.A.B. reports financial support from Kite/Gilead, Seagen, Novartis, and Nurix Therapeutics. U.F. reports financial support from Kite, a Gilead Company, MorphoSys, Caribou pharma, and Checkmate Pharma. M.K. reports financial support from AbbVie, AstraZeneca, Celgene/Bristol Myers Squibb, Adaptive Biotechnologies, ADC Therapeutics, BeiGene, Impact Bio, TG Therapeutics, Novartis, Seagen, Celgene, and Genentech. B.H. reports financial support from Viracta Therapeutics and BMS. R.K. reports financial support from Kite, BMS/Celgene, Eusa, Takeda, Pharmacyclics, Genentech/Roche, Karyopharm, BeiGene, Calithera, MorphoSys/Incyte, and AstraZeneca. J.M.V. reports financial support from AstraZeneca, Janssen, Lilly, AbbVie, Johnson & Johnson, Daiichi Sankyo, Pharmacyclics, MorphoSys, and Kite (a Gilead Company). A.J.O. reports financial support from Genmab, Precision Bio, Adaptive Biotechnologies, Celldex, Acrotech Biopharma, Schrodinger, TG Therapeutics, and Genentech. The remaining authors declare no competing financial interests.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
