

Applied coronary physiology for planning and guidance of percutaneous coronary interventions. A clinical consensus statement from the European Association of Percutaneous Cardiovascular Interventions (EAPCI) of the European Society of Cardiology
- PMID: 37171503
- PMCID: PMC10436072
- DOI: 10.4244/EIJ-D-23-00194
Applied coronary physiology for planning and guidance of percutaneous coronary interventions. A clinical consensus statement from the European Association of Percutaneous Cardiovascular Interventions (EAPCI) of the European Society of Cardiology
Abstract
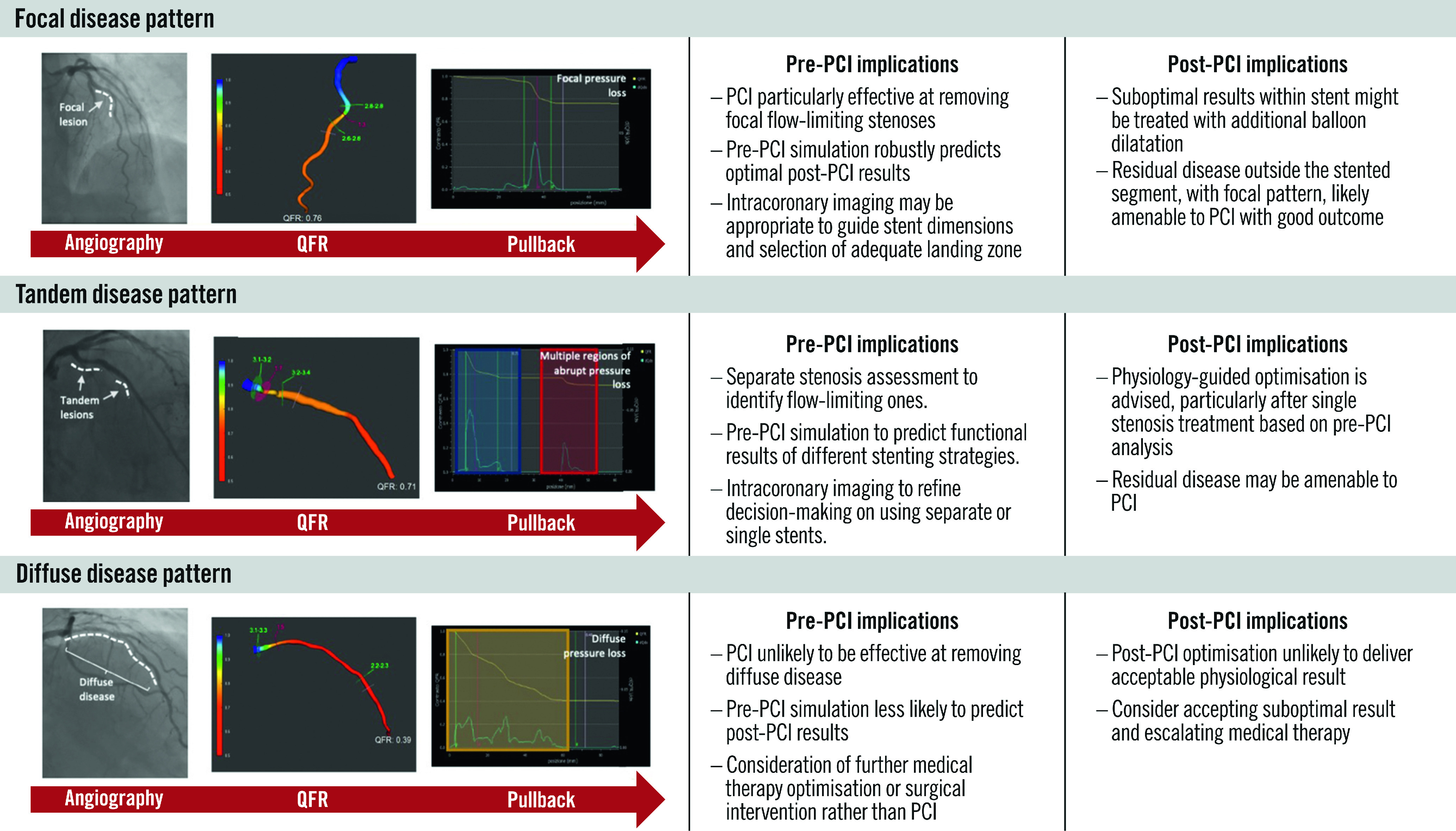
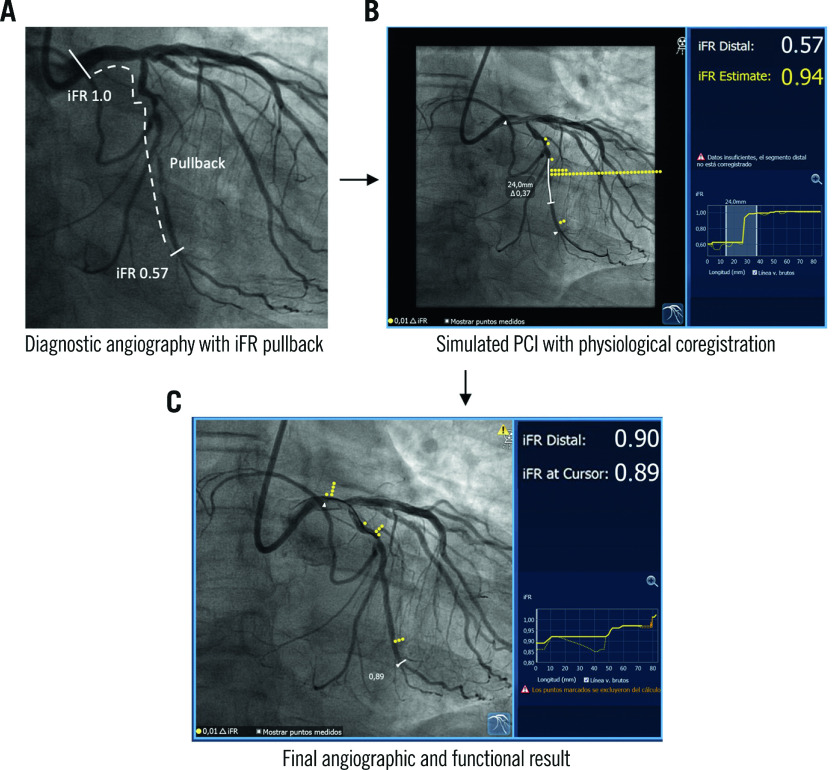
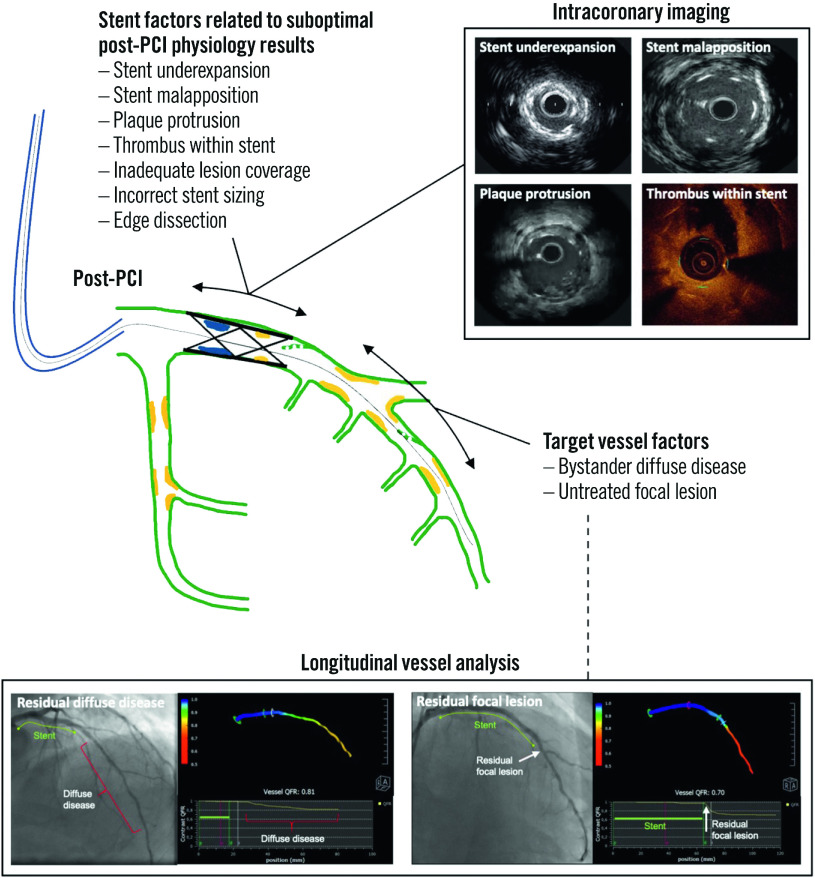
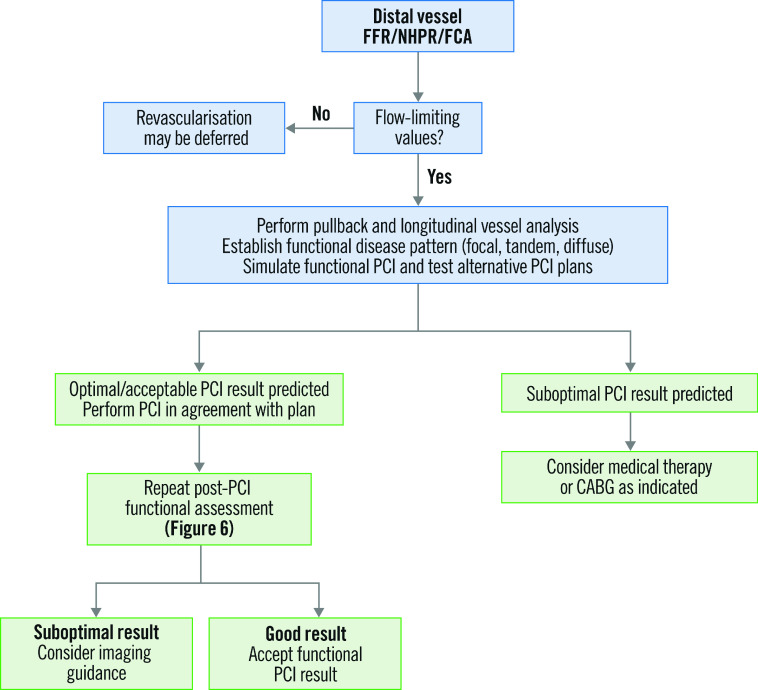
The clinical value of fractional flow reserve and non-hyperaemic pressure ratios are well established in determining an indication for percutaneous coronary intervention (PCI) in patients with coronary artery disease (CAD). In addition, over the last 5 years we have witnessed a shift towards the use of physiology to enhance procedural planning, assess post-PCI functional results, and guide PCI optimisation. In this regard, clinical studies have reported compelling data supporting the use of longitudinal vessel analysis, obtained with pressure guidewire pullbacks, to better understand how obstructive CAD contributes to myocardial ischaemia, to establish the likelihood of functionally successful PCI, to identify the presence and location of residual flow-limiting stenoses and to predict long-term outcomes. The introduction of new functional coronary angiography tools, which merge angiographic information with fluid dynamic equations to deliver information equivalent to intracoronary pressure measurements, are now available and potentially also applicable to these endeavours. Furthermore, the ability of longitudinal vessel analysis to predict the functional results of stenting has played an integral role in the evolving field of simulated PCI. Nevertheless, it is important to have an awareness of the value and challenges of physiology-guided PCI in specific clinical and anatomical contexts. The main aim of this European Association of Percutaneous Cardiovascular Interventions clinical consensus statement is to offer up-to-date evidence and expert opinion on the use of applied coronary physiology for procedural PCI planning, disease pattern recognition and post-PCI optimisation.
Conflict of interest statement
J. Escaned reports speaker or advisory board member fees from Abbott, Boston Scientific, Medis, and Philips. C. Berry is employed by the University of Glasgow, which holds consultancy and research agreements for his work with Abbott Vascular, AstraZeneca, Boehringer Ingelheim, Causeway Therapeutics, Coroventis, Genentech, GSK, HeartFlow, Menarini, Neovasc, Novartis, Siemens Healthcare, and Valo Health. B. De Bruyne reports receiving consultancy fees from Boston Scientific and Abbott Vascular; research grants from Coroventis Research, Pie Medical Imaging, CathWorks, Boston Scientific, Siemens, HeartFlow, and Abbott Vascular; and owning equity in Siemens, GE HealthCare, Philips, HeartFlow, Edwards Lifesciences, Bayer, Sanofi, and Celyad. C. Collet reports receiving research grants from Biosensor, Coroventis Research, Medis Medical Imaging, Pie Medical Imaging, CathWorks, Boston Scientific, Siemens, HeartFlow, and Abbott Vascular; and consultancy fees from HeartFlow, OpSens, Abbott Vascular, and Philips/Volcano. J.M. Lee received institutional research grants from Abbott Vascular, Boston Scientific, Terumo Corporation, Philips/Volcano, Medis Medical Imaging, and Zoll Medical. Y Appelman received speaker fees from Abbott Vascular. Si. Biscaglia received unrestricted research grants and speaker's fees from SMT, Medis, Abbott, and Insight Lifetech. P.P. Buszman is employed by the American Heart of Poland, which holds research agreements with Meril Life, and received speakers’ honoraria from Novartis. G. Campo received institutional research grants from Medis, GE HealthCare, Siemens Healthcare, Abbott Vascular, Sahajanand Medical Technologies, and Insight Lifetech. D. Collison has received consultancy and speaker fees from Abbott. A. Jeremias reports consultancy fees from Philips/Volcano, Abbott Vascular, Boston Scientific, and ACIST Medical Systems. Z. Piróth has received speakers’ fees from Abbott, Boston Scientific, and Opsens. L. Raposo has received honoraria and research grants from Philips/Volcano, St. Jude Medical (now Abbott Vascular) and HeartFlow, as well as consultancy fees from Boston Scientific. T. Rudolph received speaker honoraria from Abbott Vascular, Philips, Neovasc, AstraZeneca, Bayer, Pfizer, Philips/Volcano, Zoll Medical, and RainMed. G. Sarno has received a research grant from Boston Scientific (to the institution); and personal fees from Abbott Vascular, Boston Scientific, and Pfizer/BMS. D. Dudek reports participation in company-sponsored speaker’s bureaus for Abbott, Boston Scientific, Bracco, Philips, and Siemens Healthcare; and unrestricted grants from Abbott, Boston Scientific, Bracco, Philips, and Siemens Healthcare. The other authors have no conflicts of interest to declare.
Figures



References
-
- Knuuti J, Wijns W, Saraste A, Capodanno D, Barbato E, Funck-Brentano C, Prescott E, Storey RF, Deaton C, Cuisset T, Agewall S, Dickstein K, Edvardsen T, Escaned J, Gersh BJ, Svitil P, Gilard M, Hasdai D, Hatala R, Mahfoud F, Masip J, Muneretto C, Valgimigli M, Achenbach S, Bax JJ ESC Scientific Document Group. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur Heart J. 2020;41:407–77. - PubMed
-
- Collison D, Didagelos M, Aetesam-Ur-Rahman M, Copt S, McDade R, McCartney P, Ford TJ, McClure J, Lindsay M, Shaukat A, Rocchiccioli P, Brogan R, Watkins S, McEntegart M, Good R, Robertson K, O’Boyle P, Davie A, Khan A, Hood S, Eteiba H, Berry C, Oldroyd KG. Post-stenting fractional flow reserve vs coronary angiography for optimization of percutaneous coronary intervention (TARGET-FFR). Eur Heart J. 2021;42:4656–68. - PMC - PubMed
-
- Jeremias A, Davies JE, Maehara A, Matsumura M, Schneider J, Tang K, Talwar S, Marques K, Shammas NW, Gruberg L, Seto A, Samady H, Sharp A, Ali ZA, Mintz G, Patel M, Stone GW. Blinded Physiological Assessment of Residual Ischemia After Successful Angiographic Percutaneous Coronary Intervention: The DEFINE PCI Study. JACC Cardiovasc Interv. 2019;12:1991–2001. - PubMed
-
- Pijls NH, Klauss V, Siebert U, Powers E, Takazawa K, Fearon WF, Escaned J, Tsurumi Y, Akasaka T, Samady H, De Bruyne Fractional Flow Reserve (FFR) Post-Stent Registry Investigators. Coronary pressure measurement after stenting predicts adverse events at follow-up: a multicenter registry. Circulation. 2002;105:2950–4. - PubMed
-
- Neumann FJ, Sousa-Uva M, Ahlsson A, Alfonso F, Banning AP, Benedetto U, Byrne RA, Collet JP, Falk V, Head SJ, Jüni P, Kastrati A, Koller A, Kristensen SD, Niebauer J, Richter DJ, Seferovic PM, Sibbing D, Stefanini GG, Windecker S, Yadav R, Zembala MO ESC Scientific Document Group. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur Heart J. 2019;40:87–165. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous