

Colonoscopy surveillance in Lynch syndrome is burdensome and frequently delayed
- PMID: 37171677
- PMCID: PMC10176312
- DOI: 10.1007/s10689-023-00333-4
Colonoscopy surveillance in Lynch syndrome is burdensome and frequently delayed
Abstract
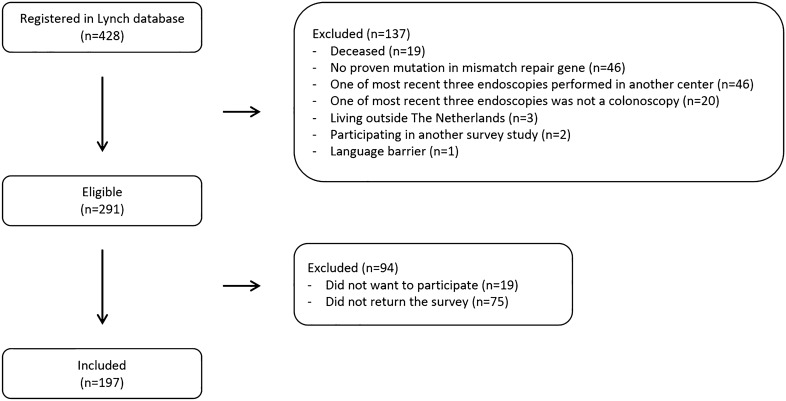
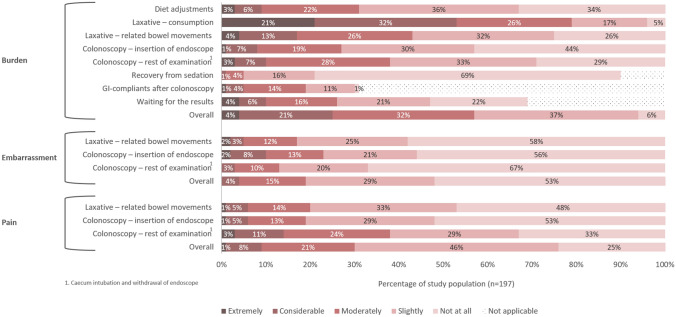
Individuals with Lynch syndrome have an increased colorectal cancer risk, hence, biennial colonoscopy surveillance is recommended. We aimed to investigate patients' perception and preferences regarding surveillance, and to further explore compliance behaviour. Individuals with Lynch syndrome received a validated survey evaluating experiences of their three most recent colonoscopies. Individuals were non-compliant to surveillance if the interval between colonoscopies differed ≥ 6 months from the recommended interval. In total, 197 of 291 (68%) invited individuals returned the survey. They mostly underwent colonoscopy biennially (99%), under mild sedation (79%) and with bowel preparation performed by Moviprep® (99%). Surveillance was perceived as impacting quality of life in 21%, and as moderately to extremely burdensome in 57%, particularly in those below age 40. To lower the burden, patients prioritised improvements in volume and taste of bowel preparation, laxation-related bowel movements, waiting times, and a more personal and respectful approach of endoscopic staff. Additionally, many individuals (60%) would favour less-invasive surveillance modalities such as biomarkers. In total, 28% of individuals had delayed colonoscopy surveillance, predominantly for patient-related reasons. An additional 10% considered quitting/postponing surveillance. Upon multivariable analysis, patient-related delay was associated with low and medium education, history of ≤ 4 colonoscopies and having no hospital recall-system. Colonoscopy surveillance in Lynch syndrome is often experienced as burdensome, and frequently delayed. We identified determinants of surveillance behaviour in this population, and present potential interventions to reduce the burden and non-compliance rates.
Keywords: Biomarker; Burden; Colonoscopy; Compliance; Lynch syndrome; Surveillance.
© 2023. The Author(s).
Conflict of interest statement
EvL, IJ and MJ have nothing to declare. ED has endoscopic equipment on a loan of FujiFilm and has received a research grant from FujiFilm. She has received an honorarium for a consultancy from FujiFilm, Olympus, InterVenn and Ambu, and speakers' fees from Olympus, GI Supply, Norgine, IPSEN, PAION and FujiFilm. NdB has served as a speaker for AbbVie and MSD and has served as a consultant and principal investigator for TEVA Pharma BV and Takeda. He has received a research grant (unrestricted) from Dr. Falk, TEVA Pharma BV, Dutch Digestive Foundation (MLDS) and Takeda. DR has received a research grant (unrestricted) from AbbVie, outside the submitted work. He has served as a member of the Data Safety Monitoring Board of Vivoryon Therapeutics.
Figures
References
-
- Monahan KJ, et al. Guidelines for the management of hereditary colorectal cancer from the British Society of Gastroenterology (BSG)/Association of Coloproctology of Great Britain and Ireland (ACPGBI)/United Kingdom Cancer Genetics Group (UKCGG) Gut. 2020;69(3):411–444. doi: 10.1136/gutjnl-2019-319915. - DOI - PMC - PubMed
-
- Vasen H, Hes F, de Jong M (2017) Dutch guideline for diagnostics and prevention of hereditary and familial tumours. https://www.stoet.nl/wp-content/uploads/2017/04/STOET-Richtlijnenboekje-...
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
