

Comparison of Maternal Labor-Related Complications and Neonatal Outcomes Following Elective Induction of Labor at 39 Weeks of Gestation vs Expectant Management: A Systematic Review and Meta-analysis
- PMID: 37171818
- PMCID: PMC10182428
- DOI: 10.1001/jamanetworkopen.2023.13162
Comparison of Maternal Labor-Related Complications and Neonatal Outcomes Following Elective Induction of Labor at 39 Weeks of Gestation vs Expectant Management: A Systematic Review and Meta-analysis
Abstract
Importance: Elective induction of labor at 39 weeks of gestation is common. Thus, there is a need to assess maternal labor-related complications and neonatal outcomes associated with elective induction of labor.
Objective: To examine maternal labor-related complications and neonatal outcomes following elective induction of labor at 39 weeks compared with expectant management.
Data sources: A systematic review of the literature was conducted using the MEDLINE (Ovid), Embase (Ovid), Cochrane Central Library, World Health Organization, and ClinicalTrials.gov databases and registries to search for articles published between database inception and December 8, 2022.
Study selection: This systematic review and meta-analysis included randomized clinical trials, cohort studies, and cross-sectional studies reporting perinatal outcomes following induction of labor at 39 weeks vs expectant management.
Data extraction and synthesis: Two reviewers independently assessed study eligibility, extracted data, and assessed studies for bias. Pooled odds ratios (ORs) and 95% CIs were calculated using a random-effects model. This study is reported per the Preferred Reporting Items for Systematic Reviews and Meta-analyses 2020 guideline, and the protocol was prospectively registered with PROSPERO.
Main outcomes and measures: Maternal outcomes of interest included emergency cesarean section, perineal injury, postpartum hemorrhage, and operative vaginal birth. Neonatal outcomes of interest included admission to the neonatal intensive care unit, low 5-minute Apgar score (<7) after birth, macrosomia, and shoulder dystocia.
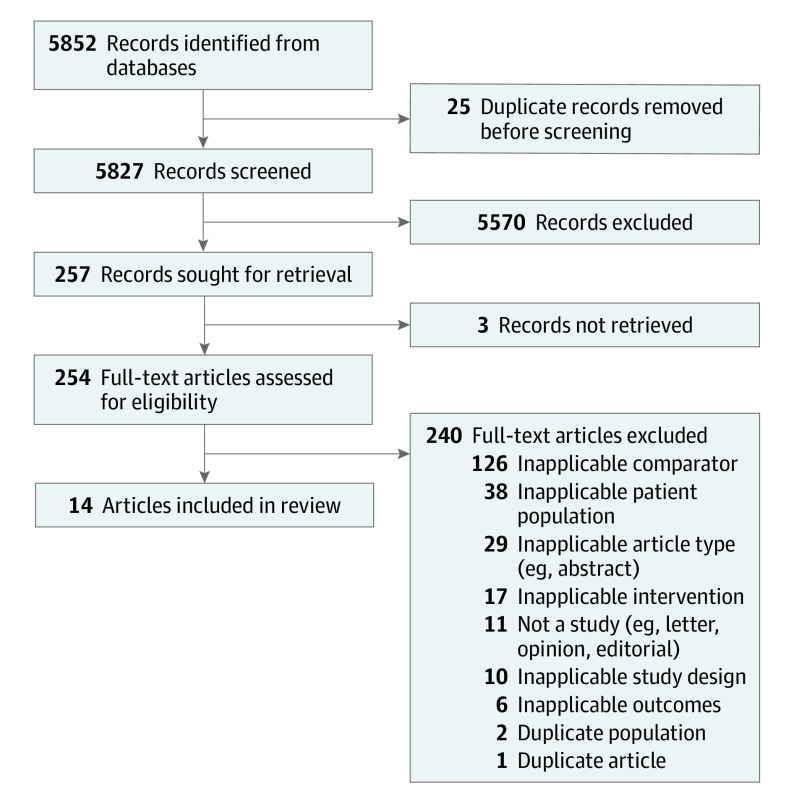
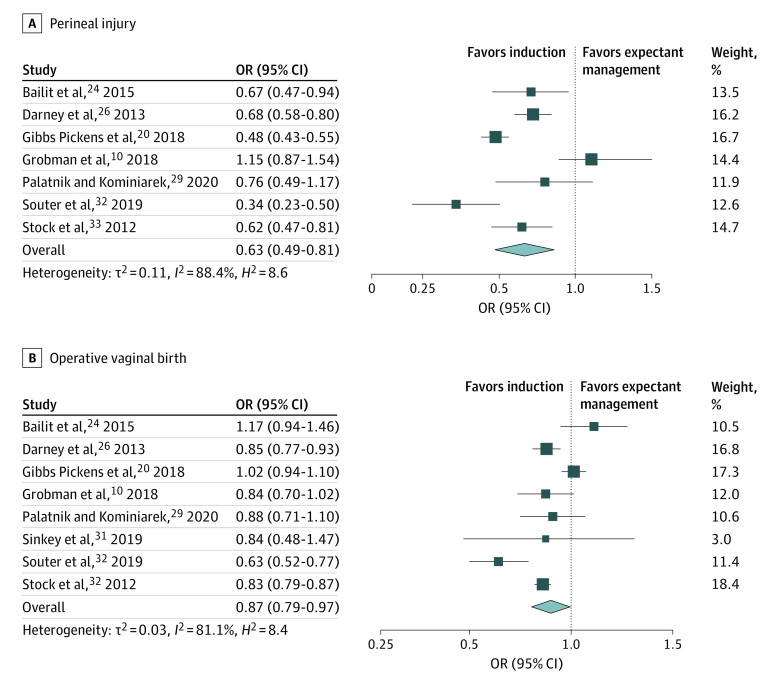
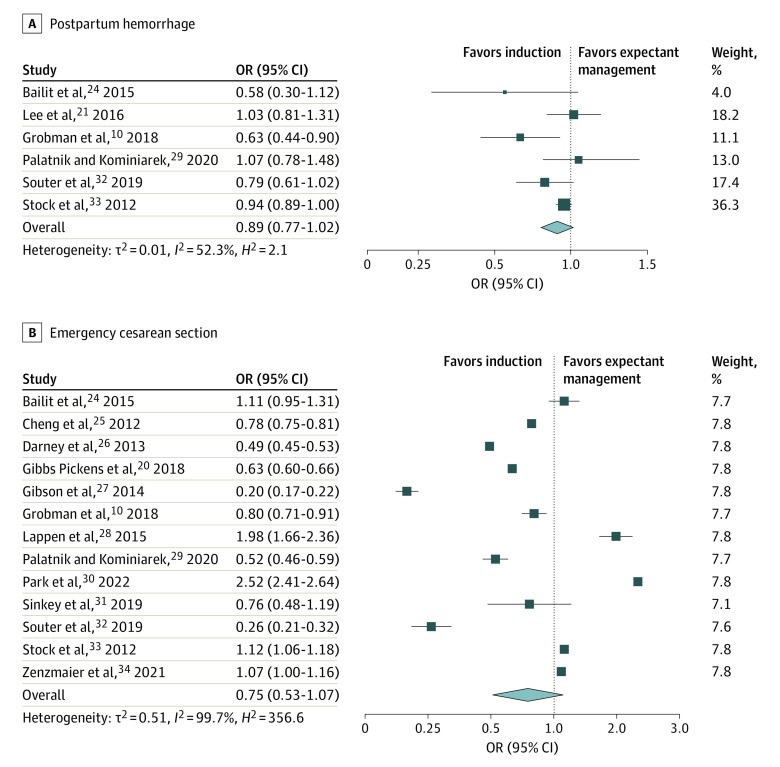
Results: Of the 5827 records identified in the search, 14 studies were eligible for inclusion in this review. These studies reported outcomes for 1 625 899 women birthing a singleton pregnancy. Induction of labor at 39 weeks of gestation was associated with a 37% reduced likelihood of third- or fourth-degree perineal injury (OR, 0.63 [95% CI, 0.49-0.81]), in addition to reductions in operative vaginal birth (OR, 0.87 [95% CI, 0.79-0.97]), macrosomia (OR, 0.66 [95% CI, 0.48-0.91]), and low 5-minute Apgar score (OR, 0.62 [95% CI, 0.40-0.96]). Results were similar when confined to multiparous women only, with the addition of a substantial reduction in the likelihood of emergency cesarean section (OR, 0.61 [95% CI, 0.38-0.98]) and no difference in operative vaginal birth (OR, 1.01 [95% CI, 0.84-1.21]). However, among nulliparous women only, induction of labor was associated with an increased likelihood of shoulder dystocia (OR, 1.22 [95% CI, 1.02-1.46]) compared with expectant management.
Conclusions and relevance: In this study, induction of labor at 39 weeks was associated with improved maternal labor-related and neonatal outcomes. However, among nulliparous women, induction of labor was associated with shoulder dystocia. These results suggest that elective induction of labor at 39 weeks may be safe and beneficial for some women; however, potential risks should be discussed with nulliparous women.
Conflict of interest statement
Figures
References
-
- National Institute for Health and Care Excellence . Inducing Labour. NICE; 2021. - PubMed
-
- Koopmans CM, Bijlenga D, Groen H, et al. ; HYPITAT Study Group . Induction of labour versus expectant monitoring for gestational hypertension or mild pre-eclampsia after 36 weeks’ gestation (HYPITAT): a multicentre, open-label randomised controlled trial. Lancet. 2009;374(9694):979-988. doi:10.1016/S0140-6736(09)60736-4 - DOI - PubMed
-
- World Health Organization . WHO recommendations for induction of labour. 2011. Accessed February 2, 2023. https://www.who.int/publications/i/item/9789241501156 - PubMed
-
- World Health Organization . WHO recommendations: induction of labour at or beyond term. 2018. Accessed February 2, 2023. https://apps.who.int/iris/bitstream/handle/10665/277233/9789241550413-en... - PubMed
-
- Wennerholm UB, Saltvedt S, Wessberg A, et al. . Induction of labour at 41 weeks versus expectant management and induction of labour at 42 weeks (SWEdish Post-term Induction Study, SWEPIS): multicentre, open label, randomised, superiority trial. BMJ. 2019;367:l6131. doi:10.1136/bmj.l6131 - DOI - PMC - PubMed
