

Obstetric and neonatal outcomes after natural versus artificial cycle frozen embryo transfer and the role of luteal phase support: a systematic review and meta-analysis
- PMID: 37172270
- PMCID: PMC10477943
- DOI: 10.1093/humupd/dmad011
Obstetric and neonatal outcomes after natural versus artificial cycle frozen embryo transfer and the role of luteal phase support: a systematic review and meta-analysis
Abstract
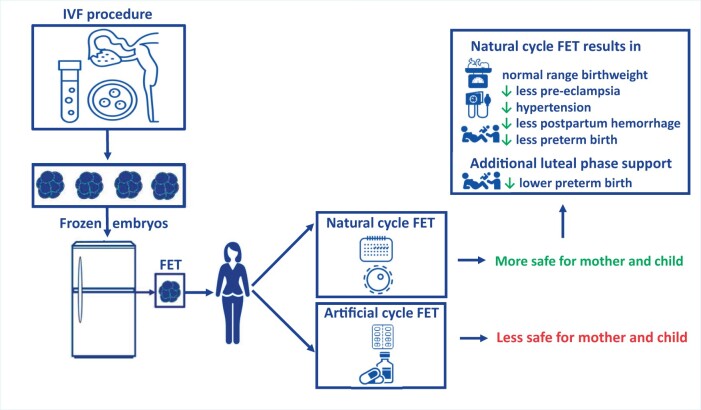
Background: The number of frozen embryo transfers (FET) has increased dramatically over the past decade. Based on current evidence, there is no difference in pregnancy rates when natural cycle FET (NC-FET) is compared to artificial cycle FET (AC-FET) in subfertile women. However, NC-FET seems to be associated with lower risk of adverse obstetric and neonatal outcomes compared with AC-FET cycles. Currently, there is no consensus about whether NC-FET needs to be combined with luteal phase support (LPS) or not. The question of how to prepare the endometrium for FET has now gained even more importance and taken the dimension of safety into account as it should not simply be reduced to the basic question of effectiveness.
Objective and rationale: The objective of this project was to determine whether NC-FET, with or without LPS, decreases the risk of adverse obstetric and neonatal outcomes compared with AC-FET.
Search methods: A systematic review and meta-analysis was carried out. A literature search was performed using the following databases: CINAHL, EMBASE, and MEDLINE from inception to 10 October 2022. Observational studies, including cohort studies, and registries comparing obstetric and neonatal outcomes between singleton pregnancies after NC-FET and those after AC-FET were sought. Risk of bias was assessed using the ROBINS-I tool. The quality of evidence was evaluated using the Grading of Recommendations Assessment, Development and Evaluation approach. We calculated pooled odds ratios (ORs), pooled risk differences (RDs), pooled adjusted ORs, and prevalence estimates with 95% CI using a random effect model, while heterogeneity was assessed by the I2.
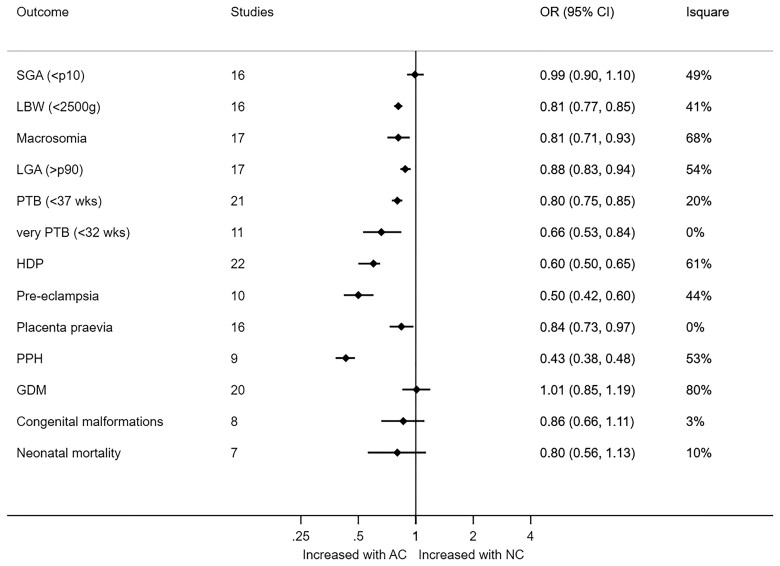
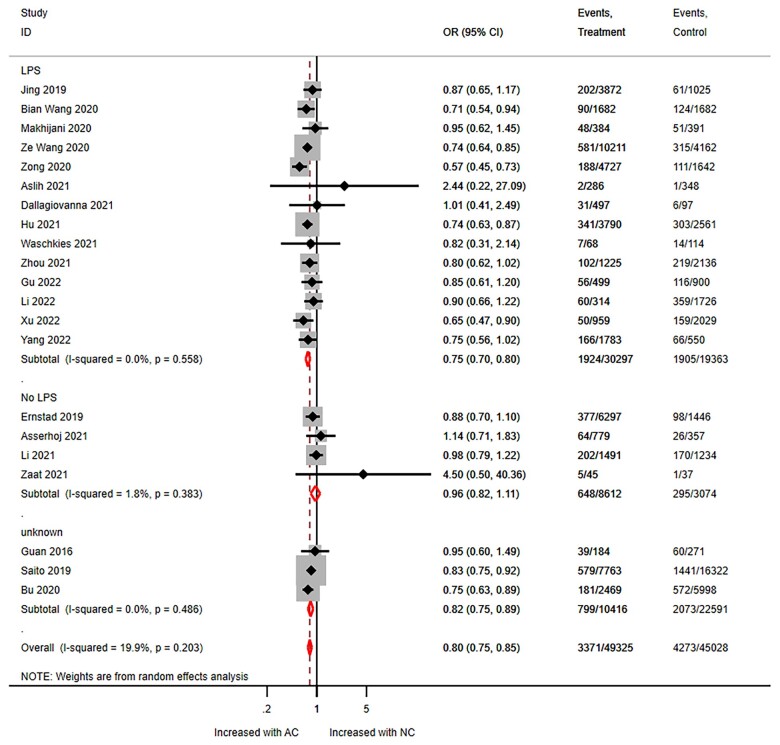
Outcomes: The conducted search identified 2436 studies, 890 duplicates were removed and 1546 studies were screened. Thirty studies (NC-FET n = 56 445; AC-FET n = 57 231) were included, 19 of which used LPS in NC-FET. Birthweight was lower following NC-FET versus AC-FET (mean difference 26.35 g; 95% CI 11.61-41.08, I2 = 63%). Furthermore NC-FET compared to AC-FET resulted in a lower risk of large for gestational age (OR 0.88, 95% 0.83-0.94, I2 = 54%), macrosomia (OR 0.81; 95% CI 0.71-0.93, I2 = 68%), low birthweight (OR 0.81, 95% CI 0.77-0.85, I2 = 41%), early pregnancy loss (OR 0.73; 95% CI 0.61-0.86, I2 = 70%), preterm birth (OR 0.80; 95% CI 0.75-0.85, I2 = 20%), very preterm birth (OR 0.66, 95% CI 0.53-0.84, I2 = 0%), hypertensive disorders of pregnancy (OR 0.60, 95% CI 0.50-0.65, I2 = 61%), pre-eclampsia (OR 0.50; 95% CI 0.42-0.60, I2 = 44%), placenta previa (OR 0.84, 95% CI 0.73-0.97, I2 = 0%), and postpartum hemorrhage (OR 0.43; 95% CI 0.38-0.48, I2 = 53%). Stratified analyses on LPS use in NC-FET suggested that, compared to AC-FET, NC-FET with LPS decreased preterm birth risk, while NC-FET without LPS did not (OR 0.75, 95% CI 0.70-0.81). LPS use did not modify the other outcomes. Heterogeneity varied from low to high, while quality of the evidence was very low to moderate.
Wider implications: This study confirms that NC-FET decreases the risk of adverse obstetric and neonatal outcomes compared with AC-FET. We estimate that for each adverse outcome, use of NC-FET may prevent 4 to 22 cases per 1000 women. Consequently, NC-FET should be the preferred treatment in women with ovulatory cycles undergoing FET. Based on very low quality of evidence, the risk of preterm birth be decreased when LPS is used in NC-FET compared to AC-FET. However, because of many uncertainties-the major being the debate about efficacy of the use of LPS-future research is needed on efficacy and safety of LPS and no recommendation can be made about the use of LPS.
Keywords: artificial cycle; birthweight; frozen-thawed embryo transfer; hypertensive disorders of pregnancy; luteal phase support; natural cycle; safety.
© The Author(s) 2023. Published by Oxford University Press on behalf of European Society of Human Reproduction and Embryology.
Conflict of interest statement
T.R.Z. is supported by a grant of the Netherlands Organisation for Health Research and Development (ZonMw 843002807) in order to perform the The Antarctica-2 RCT (Trial NL6414 (NTR6590)).
All reported competing interests are outside the submitted work. No other relationships or activities that could appear to have influenced the submitted work. The remaining authors have no conflicts of interest to declare.
Figures



Comment in
-
Reply: Artificial cycle frozen embryo transfer and obstetric adverse outcomes: association or causation?Hum Reprod Update. 2023 Sep 5;29(5):697. doi: 10.1093/humupd/dmad021. Hum Reprod Update. 2023. PMID: 37507139 No abstract available.
-
Artificial cycle frozen embryo transfer and obstetric adverse outcomes: association or causation?Hum Reprod Update. 2023 Sep 5;29(5):694-696. doi: 10.1093/humupd/dmad020. Hum Reprod Update. 2023. PMID: 37507148 No abstract available.
References
-
- American College of Obstetricians and Gynecologists’ Committee on Practice Bulletins—Obstetrics. Prediction and prevention of spontaneous preterm birth: ACOG Practice Bulletin, Number 234. Obstet Gynecol 2021;138:e65–e90. - PubMed
-
- Asserhoj LL, Spangmose AL, Aaris Henningsen AK, Clausen TD, Ziebe S, Jensen RB, Pinborg A.. Adverse obstetric and perinatal outcomes in 1,136 singleton pregnancies conceived after programmed frozen embryo transfer (FET) compared with natural cycle FET. Fertil Steril 2021;115:947–956. - PubMed
-
- Atkins D, Eccles M, Flottorp S, Guyatt GH, Henry D, Hill S, Liberati A, O'Connell D, Oxman AD, Phillips B. et al. ; GRADE Working Group. Systems for grading the quality of evidence and the strength of recommendations I: critical appraisal of existing approaches The GRADE Working Group. BMC Health Serv Res 2004;4:38. - PMC - PubMed
-
- Audette MC, Kingdom JC.. Screening for fetal growth restriction and placental insufficiency. Semin Fetal Neonatal Med 2018;23:119–125. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
