

Interventional therapies for pulmonary embolism
- PMID: 37173409
- PMCID: PMC10180624
- DOI: 10.1038/s41569-023-00876-0
Interventional therapies for pulmonary embolism
Abstract
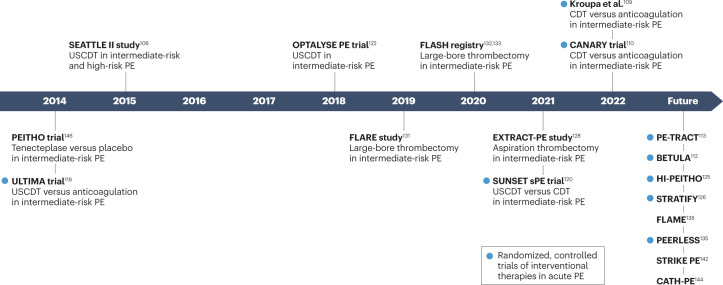
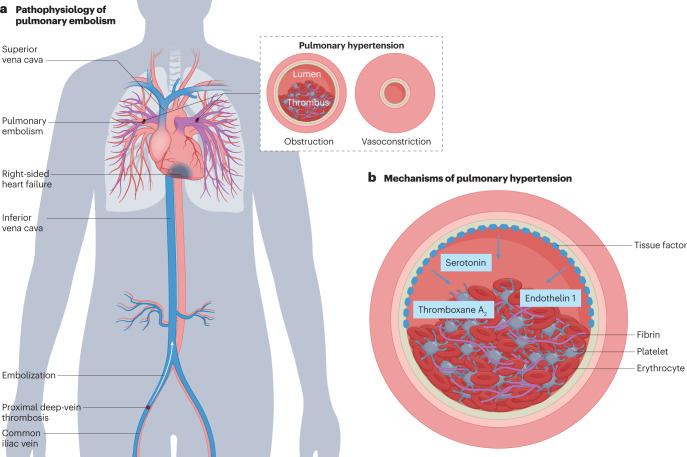
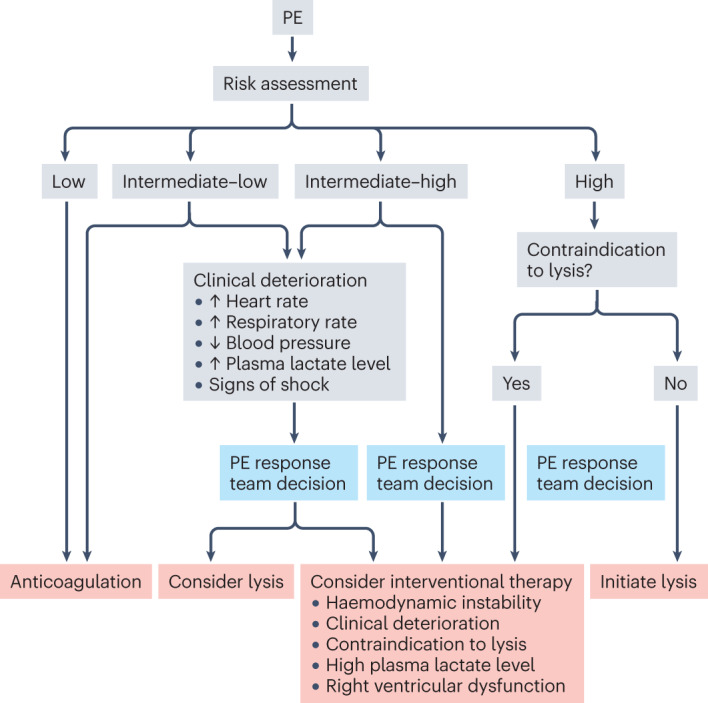
Pulmonary embolism (PE) is the leading cause of in-hospital death and the third most frequent cause of cardiovascular death. The clinical presentation of PE is variable, and choosing the appropriate treatment for individual patients can be challenging. Traditionally, treatment of PE has involved a choice of anticoagulation, thrombolysis or surgery; however, a range of percutaneous interventional technologies have been developed that are under investigation in patients with intermediate-high-risk or high-risk PE. These interventional technologies include catheter-directed thrombolysis (with or without ultrasound assistance), aspiration thrombectomy and combinations of the aforementioned principles. These interventional treatment options might lead to a more rapid improvement in right ventricular function and pulmonary and/or systemic haemodynamics in particular patients. However, evidence from randomized controlled trials on the safety and efficacy of these interventions compared with conservative therapies is lacking. In this Review, we discuss the underlying pathophysiology of PE, provide assistance with decision-making on patient selection and critically appraise the available clinical evidence on interventional, catheter-based approaches for PE treatment. Finally, we discuss future perspectives and unmet needs.
© 2023. Springer Nature Limited.
Conflict of interest statement
F.G. has received speaker honoraria from AstraZeneca. L.L. has received speaker honoraria from Medtronic and ReCor Medical. I.M.L. has relationships with the following drug companies: Actelion-Janssen, AOP-Health, Ferrer, Medtronic, MSD, Neutrolis and United Therapeutics; in addition to being an investigator in trials involving these companies, relationships include consultancy services, research grants and membership of scientific advisory boards. S.R. has received fees for lectures and/or consultations from Abbott, Acceleron, Actelion, Aerovate, Altavant, AOP Orphan, AstraZeneca, Bayer, Boehringer Ingelheim, Edwards, Ferrer, Gossamer, Janssen, MSD, United Therapeutics and Vifor; his institution has received research grants from Actelion, AstraZeneca, Bayer and Janssen. S.K. reports grants or contracts from Bayer, Boston Scientific and Daiichi Sankyo, and consulting and lecture fees from Bayer, Boston Scientific, Daiichi Sankyo, MSD and Pfizer–Bristol-Myers Squibb. M.B. is supported by Abbott, Amgen, AstraZeneca, Bayer, Boehringer Ingelheim, Bristol Myers Squibb, Medtronic, Novartis, ReCor Medical, Servier and Vifor. W.J. is a consultant for Inari Medical and Medtronic. F.M. has received scientific support from Ablative Solutions, Medtronic and ReCor Medical and speaker honoraria/consulting fees from Ablative Solutions, Amgen, AstraZeneca, Bayer, Boehringer Ingelheim, Inari, Medtronic, Merck, ReCor Medical, Servier and Terumo. The other authors declare no competing interests.
Figures

References
-
- Heit JA, Cohen AT, Anderson FA. Estimated annual number of incident and recurrent, non-fatal and fatal venous thromboembolism (VTE) events in the US. Blood. 2005;106:910–910. doi: 10.1182/blood.V106.11.910.910. - DOI
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
