

Long-term safety and maintenance of response with esketamine nasal spray in participants with treatment-resistant depression: interim results of the SUSTAIN-3 study
- PMID: 37173512
- PMCID: PMC10267177
- DOI: 10.1038/s41386-023-01577-5
Long-term safety and maintenance of response with esketamine nasal spray in participants with treatment-resistant depression: interim results of the SUSTAIN-3 study
Abstract
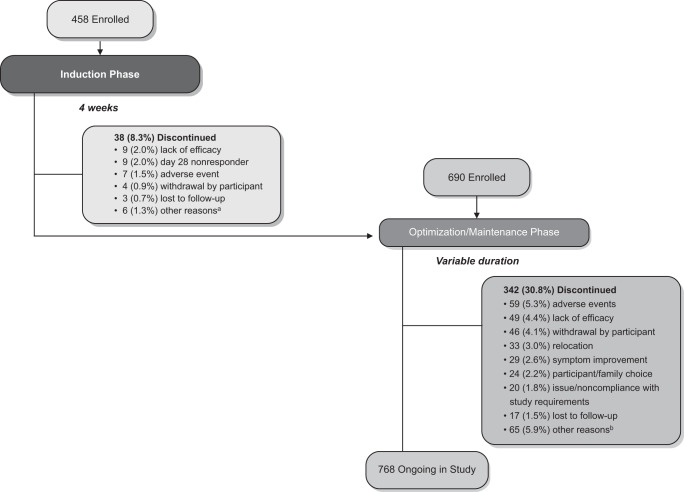
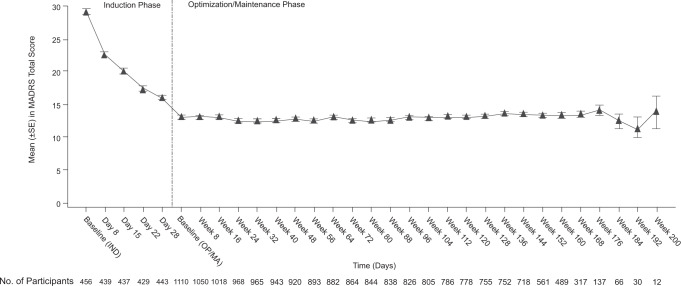
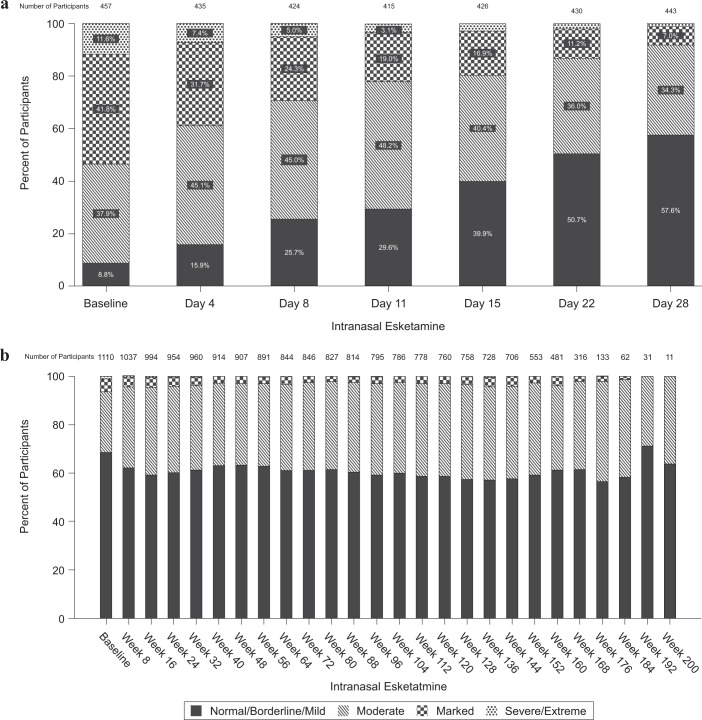
Patients with treatment-resistant depression (TRD) have higher rates of relapse and pronounced decreases in daily functioning and health-related quality of life compared to patients with major depressive disorder who are not treatment-resistant, underscoring the need for treatment choices with sustained efficacy and long-term tolerability. Adults with TRD who participated in ≥1 of 6 phase 3 "parent" studies could continue esketamine treatment, combined with an oral antidepressant, by enrolling in phase 3, open-label, long-term extension study, SUSTAIN-3. Based on their status at parent-study end, eligible participants entered a 4-week induction phase followed by an optimization/maintenance phase, or directly entered the optimization/maintenance phase of SUSTAIN-3. Intranasal esketamine dosing was flexible, twice-weekly during induction and individualized to depression severity during optimization/maintenance. At the interim data cutoff (01 December 2020), 1148 participants were enrolled, 458 at induction and 690 at optimization/maintenance. Mean (median) cumulative duration of maintenance esketamine treatment was 31.5 (37.7) months (totaling 2769 cumulative patient-years). Common treatment-emergent adverse events (≥20%) were headache, dizziness, nausea, dissociation, somnolence, and nasopharyngitis. Mean Montgomery-Åsberg Depression Rating Scale (MADRS) total score decreased during induction, and this reduction persisted during optimization/maintenance (mean [SD] change from the baseline to the endpoint of each phase: induction -12.8 [9.73]; optimization/maintenance +1.1 [9.93]), with 35.6% and 46.1% of participants in remission (MADRS total score ≤12) at induction and optimization/maintenance endpoints, respectively. Improvement in depression ratings generally persisted among participants who remained in maintenance treatment, and no new safety signal was identified during long-term treatment (up to 4.5 years) using intermittent-dosed esketamine in conjunction with daily antidepressant.
Trial registration: ClinicalTrials.gov NCT02782104.
© 2023. Janssen Research & Development, LLC.
Conflict of interest statement
NZ, LC, TD, WCD, VP, D-JF, and RL are employees of Janssen Research & Development, LLC or Janssen Research & Development Belgium, and all are stockholders of Johnson & Johnson. RLM was an employee of Janssen Research & Development, LLC at the time this work was conducted. In the last 12 months. GS has provided consulting services to Ancora, Aptinyx, Axsome Therapeutics, Biohaven Pharmaceuticals, Bristol-Myers Squibb, Clexio Biosciences, Denovo Biopharma, EMA Wellness, Engrail, Gilgamesh, Freedom Biosciences, Intra-Cellular Therapies, Janssen, miCure Therapeutics, Merck, Navitor Pharmaceuticals, Neurocrine, Novartis, Noven Pharmaceuticals, Perception Neuroscience, Praxis, Sage Pharmaceuticals, Seelos Pharmaceuticals, and XW Labs. He has received funds for contracted research from Janssen Pharmaceuticals, Merck, and Usona Institute. He holds equity in Biohaven Pharmaceuticals and has received royalties paid from patent licenses with Biohaven Pharmaceuticals. His employer, Yale University, has a financial relationship with Janssen Pharmaceuticals and may receive financial benefits from this relationship. STW has received contract funding for clinical trials from Sage Therapeutics, Oui Therapeutics, and Janssen (administered through Yale University). He has received consulting fees from Sage Therapeutics, Oui Therapeutics, and Janssen.
Figures
References
-
- American Psychiatric Association. Practice Guideline for the Treatment of Patients with Major Depressive Disorder, 3rd ed. American Psychiatric Association: Washington, DC; 2013. https://psychiatryonline.org/pb/assets/raw/sitewide/practice_guidelines/.... Accessed 18 September 2022.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
