

Thromboelastographic evaluation after cardiac surgery optimizes transfusion requirements in the intensive care unit: a single-center retrospective cohort study using an inverse probability weighting method
- PMID: 37173610
- PMCID: PMC10180616
- DOI: 10.1007/s11748-023-01941-8
Thromboelastographic evaluation after cardiac surgery optimizes transfusion requirements in the intensive care unit: a single-center retrospective cohort study using an inverse probability weighting method
Abstract
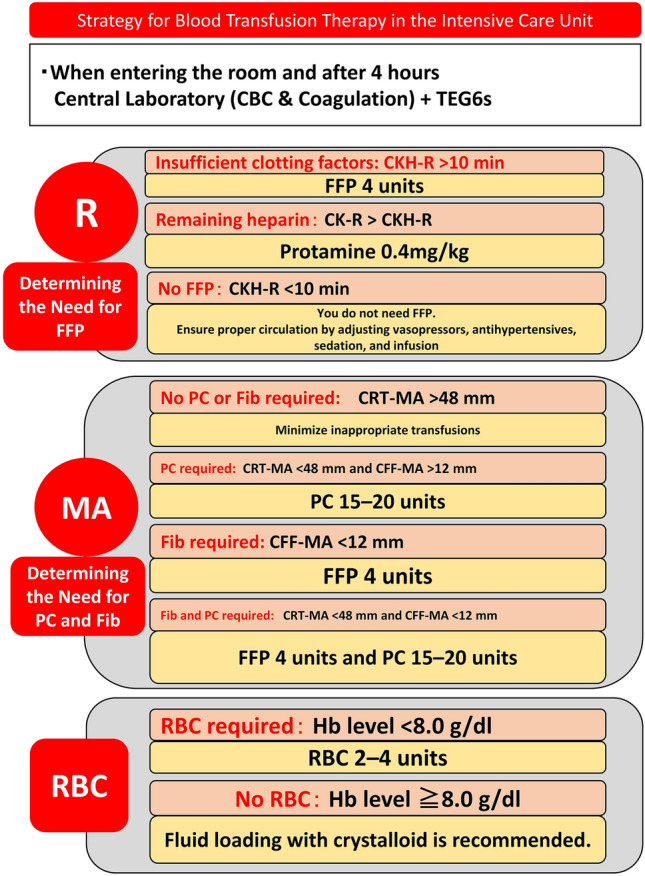
Objective: There are no reports from Japan showing the effects of using the thromboelastography algorithm on transfusion requirements after Intensive Care Unit (ICU) admission, and post-implementation knowledge regarding the thromboelastography algorithm under the Japanese healthcare system is insufficient. Therefore, this study aimed to clarify the effect of the TEG6s thromboelastography algorithm on transfusion requirements for patients in the ICU after cardiac surgery.
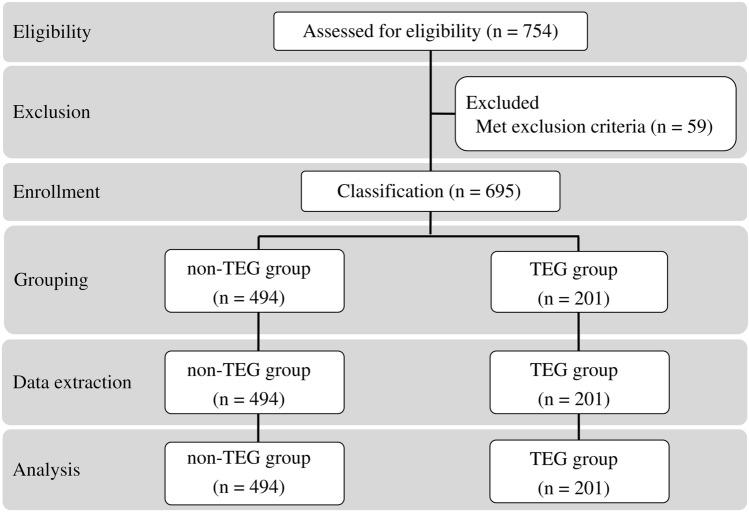
Methods: We retrospectively compared the requirements for blood transfusion up to 24 h after ICU admission using the thromboelastography algorithm (January 2021 to April 2022) (thromboelastography group; n = 201) and specialist consultation with surgeons and anesthesiologists (January 2018 to December 2020) (non-thromboelastography group; n = 494).
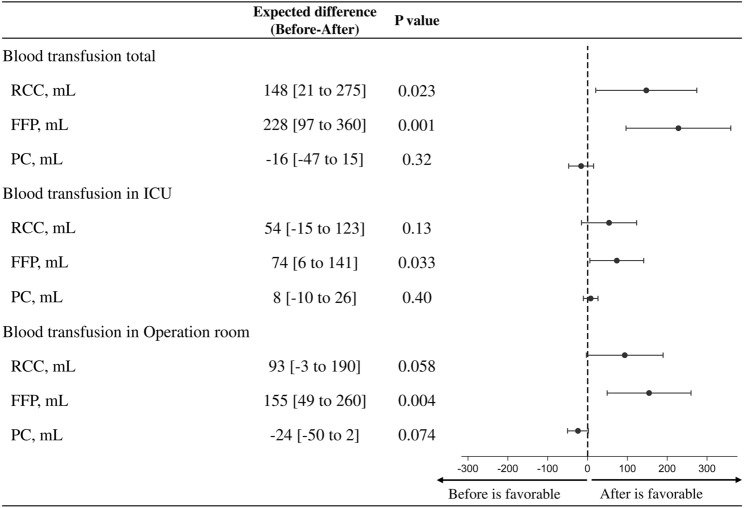
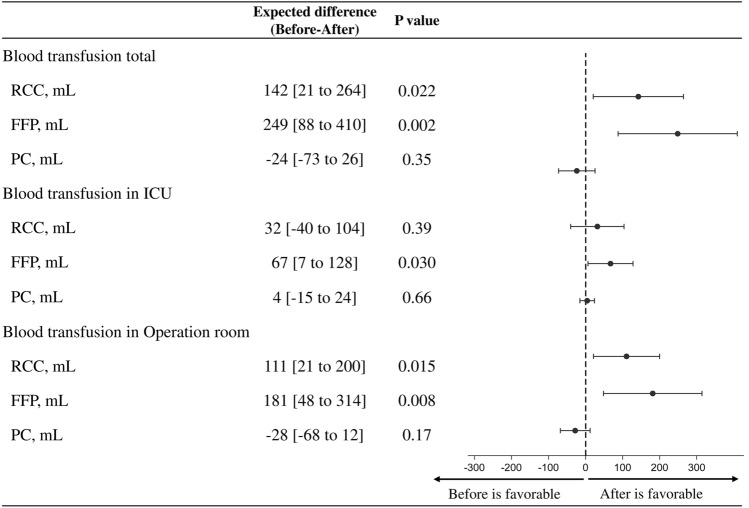
Results: There were no significant between-group differences in terms of age, height, weight, body mass index, operative procedure, duration of surgery or cardiopulmonary bypass, body temperature, or urine volume during surgical intervention. Moreover, there was no significant between-group difference in the amount of drainage at 24 h after ICU admission. However, crystalloid and urine volumes were significantly higher in the thromboelastography group than in the non-thromboelastography group. Additionally, fresh-frozen plasma (FFP) transfusion volumes were significantly lower in the thromboelastography group. However, there were no significant between-group differences in red blood cell count or platelet transfusion volume. After variable adjustment, the amount of FFP used from the operating room to 24 h after ICU admission was significantly reduced in the thromboelastography group.
Conclusions: The thromboelastography algorithm optimized transfusion requirements at 24 h after admission to the ICU following cardiac surgery.
Keywords: Cardiac surgery; Intensive care unit; Patient blood management; Thromboelastography; Transfusion.
© 2023. The Author(s), under exclusive licence to The Japanese Association for Thoracic Surgery.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures
Similar articles
-
Thromboelastography-guided transfusion algorithm reduces transfusions in complex cardiac surgery.Anesth Analg. 1999 Feb;88(2):312-9. doi: 10.1097/00000539-199902000-00016. Anesth Analg. 1999. PMID: 9972747 Clinical Trial.
-
Transfusion requirements in elective cardiopulmonary bypass surgery patients: predictive value of Multiplate and Thromboelastography (TEG) Platelet Mapping Assay.Scand J Clin Lab Invest. 2017 Sep;77(5):345-351. doi: 10.1080/00365513.2017.1325000. Epub 2017 May 24. Scand J Clin Lab Invest. 2017. PMID: 28537454
-
Thromboelastography Is Associated With Surrogates for Bleeding After Pediatric Cardiac Operations.Ann Thorac Surg. 2018 Sep;106(3):799-806. doi: 10.1016/j.athoracsur.2018.04.023. Epub 2018 May 16. Ann Thorac Surg. 2018. PMID: 29753821
-
Thromboelastography-guided therapy improves patient blood management and certain clinical outcomes in elective cardiac and liver surgery and emergency resuscitation: A systematic review and analysis.J Thromb Haemost. 2019 Jun;17(6):984-994. doi: 10.1111/jth.14447. Epub 2019 May 13. J Thromb Haemost. 2019. PMID: 30947389 Free PMC article.
-
Roles of thrombelastography and thromboelastometry for patient blood management in cardiac surgery.Transfus Med Rev. 2013 Oct;27(4):213-20. doi: 10.1016/j.tmrv.2013.08.004. Epub 2013 Sep 26. Transfus Med Rev. 2013. PMID: 24075802 Review.
Cited by
-
The impact of the patient's plasma volume on the amount of fresh frozen plasma needed to normalize the thromboelastographic reaction time.Eur J Trauma Emerg Surg. 2025 May 2;51(1):191. doi: 10.1007/s00068-025-02870-2. Eur J Trauma Emerg Surg. 2025. PMID: 40316863
-
Use of Thromboelastography in Coronary Artery Bypass Grafting in a Patient With Factor Ⅴ Deficiency With Platelet Function Disorders: A Case Report and Literature Review.Cureus. 2024 Apr 13;16(4):e58185. doi: 10.7759/cureus.58185. eCollection 2024 Apr. Cureus. 2024. PMID: 38741825 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
