

Effect of emergency physician-operated emergency short-stay ward on emergency department stay length and clinical outcomes: a case-control study
- PMID: 37173654
- PMCID: PMC10176288
- DOI: 10.1186/s12873-023-00813-x
Effect of emergency physician-operated emergency short-stay ward on emergency department stay length and clinical outcomes: a case-control study
Abstract
Background: We hypothesized that an emergency short-stay ward (ESSW) mainly operated by emergency medicine physicians may reduce the length of patient stay in emergency department without expense of clinical outcomes.
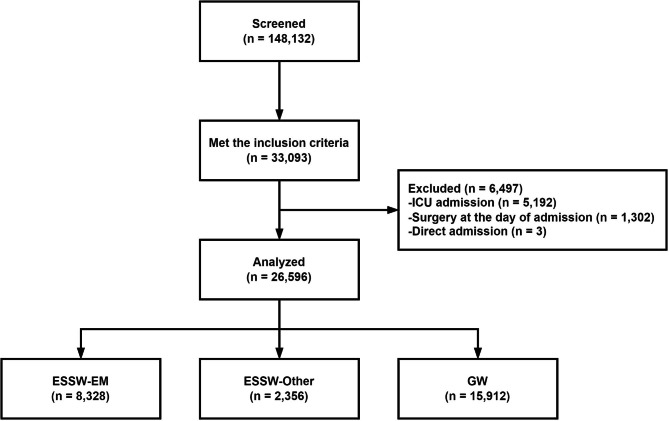
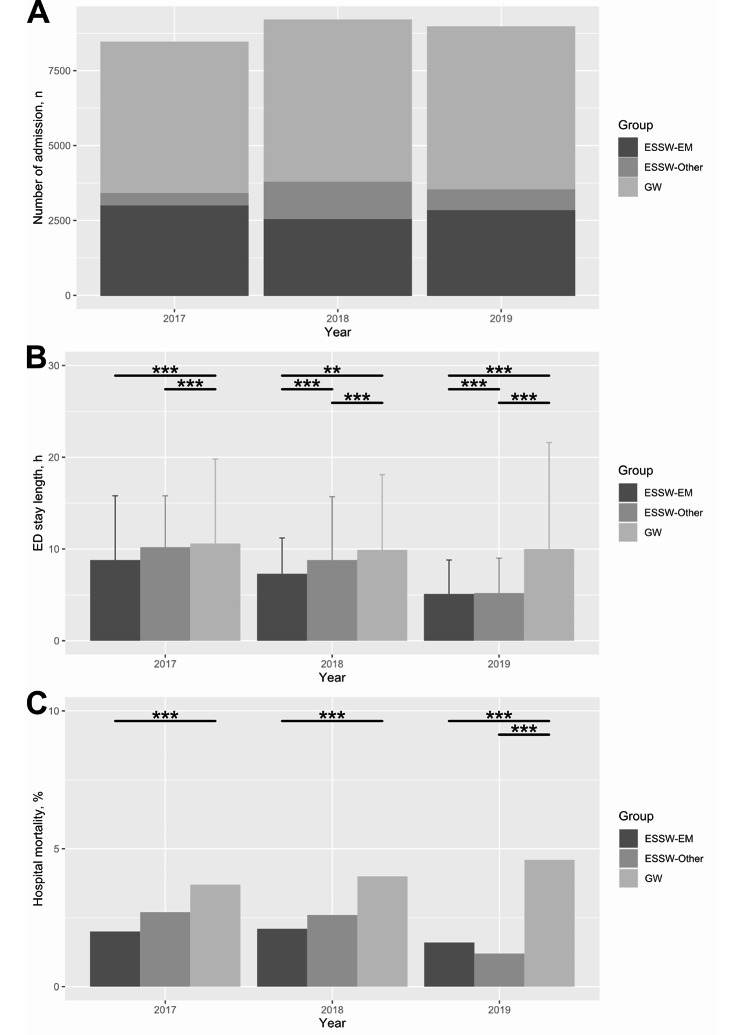
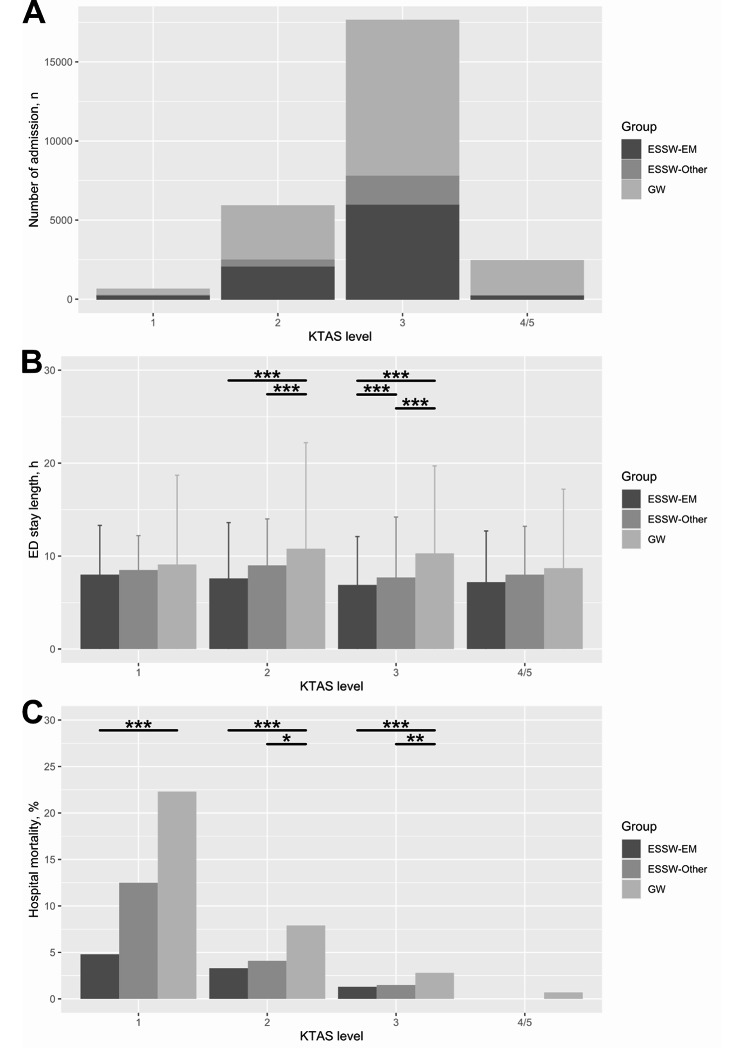
Methods: We retrospectively analysed adult patients who visited the emergency department of the study hospital and were subsequently admitted to wards from 2017 to 2019. We divided study participants into three groups: patients admitted to ESSW and treated by the department of emergency medicine (ESSW-EM), patients admitted to ESSW and treated by other departments (ESSW-Other) and patients admitted to general wards (GW). The co-primary outcomes were ED length of stay and 28-day hospital mortality.
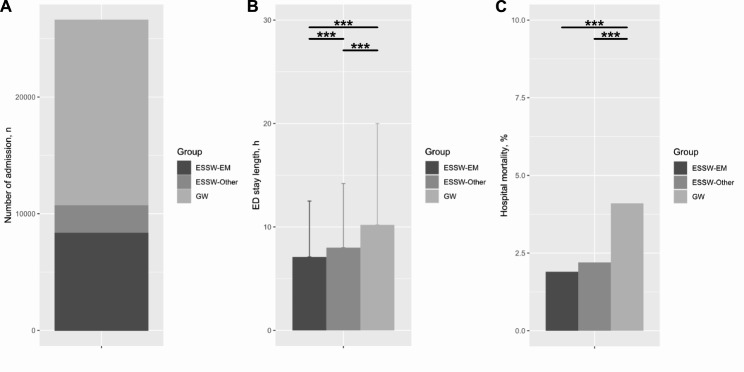
Results: In total, 29,596 patients were included in the study, and 8,328 (31.3%), 2,356 (8.9%), and 15,912 (59.8%) of them were classified as ESSW-EM, ESSW-Other and GW groups, respectively. The ED length of stay of the ESSW-EM (7.1 h ± 5.4) was shorter than those of the ESSW-Other (8.0 ± 6.2, P < 0.001) and the GW (10.2 ± 9.8, P < 0.001 for both). Hospital mortality of ESSW-EM (1.9%) was lower than that of GW (4.1%, P < 0.001). In the multivariable linear regression analysis, the ESSW-EM was independently associated with shorter ED length of stay compared with the both ESSW-Other (coefficient, 1.08; 95% confidence interval, 0.70-1.46; P < 0.001) and GW (coefficient, 3.35; 95% confidence interval, 3.12-3.57; P < 0.001). In the multivariable logistic regression analyses, the ESSW-EM was independently associated with lower hospital mortality compared with both the ESSW-Other group (adjusted P = 0.030) and the GW group (adjusted P < 0.001).
Conclusions: In conclusion, the ESSW-EM was independently associated with shorter ED length of stay compared with both the ESSW-Other and the GW in the adult ED patients. Independent association was found between the ESSW-EM and lower hospital mortality compared with the GW.
Keywords: Emergency Department; Emergency Short-Stay ward; Length of stay.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Emergency short-stay wards and boarding time in emergency departments: A propensity-score matching study.Am J Emerg Med. 2020 Dec;38(12):2495-2499. doi: 10.1016/j.ajem.2019.12.014. Epub 2019 Dec 9. Am J Emerg Med. 2020. PMID: 31859191
-
Medical expertise as a critical influencing factor on the length of stay in the ED: A retrospective cohort study.Medicine (Baltimore). 2021 May 14;100(19):e25911. doi: 10.1097/MD.0000000000025911. Medicine (Baltimore). 2021. PMID: 34106655 Free PMC article.
-
The effect of direct admission to acute geriatric units compared to admission after an emergency department visit on length of stay, postacute care transfers and ED return visits.BMC Geriatr. 2022 Jul 4;22(1):555. doi: 10.1186/s12877-022-03241-x. BMC Geriatr. 2022. PMID: 35788184 Free PMC article.
-
Who is less likely to die in association with improved National Emergency Access Target (NEAT) compliance for emergency admissions in a tertiary referral hospital?Aust Health Rev. 2016 Apr;40(2):149-154. doi: 10.1071/AH14242. Aust Health Rev. 2016. PMID: 26278814
-
Emergency Department disposition decisions and associated mortality and costs in ICU patients with suspected infection.Crit Care. 2018 Jul 6;22(1):172. doi: 10.1186/s13054-018-2096-8. Crit Care. 2018. PMID: 29976238 Free PMC article.
Cited by
-
Shortening emergency department length of stay: Fast track, short-stay unit and acute medical unit.Explor Res Clin Soc Pharm. 2025 Jun 19;19:100626. doi: 10.1016/j.rcsop.2025.100626. eCollection 2025 Sep. Explor Res Clin Soc Pharm. 2025. PMID: 40678677 Free PMC article. Review.
References
-
- Yoon BS, Choa MH, Kong TY, Joo YS, Ko DR, Hwang YJ, et al. The effect of time target on overcrowding and clinical quality in the ED: a systematic review and meta-analysis. J Korean Soc Emerg Med. 2018;29(2):170–8.
MeSH terms
LinkOut - more resources
Full Text Sources
