

Comparison of ductus venosus Doppler and cerebroplacental ratio for the prediction of adverse perinatal outcome in high-risk pregnancies before and after 34 weeks
- PMID: 37173867
- PMCID: PMC10333667
- DOI: 10.1111/aogs.14570
Comparison of ductus venosus Doppler and cerebroplacental ratio for the prediction of adverse perinatal outcome in high-risk pregnancies before and after 34 weeks
Abstract
Introduction: The objective of the study was to compare the accuracy of the ductus venosus pulsatility index (DV PI) with that of the cerebroplacental ratio (CPR) for the prediction of adverse perinatal outcome at two gestational ages: <34 and ≥34 weeks' gestation.
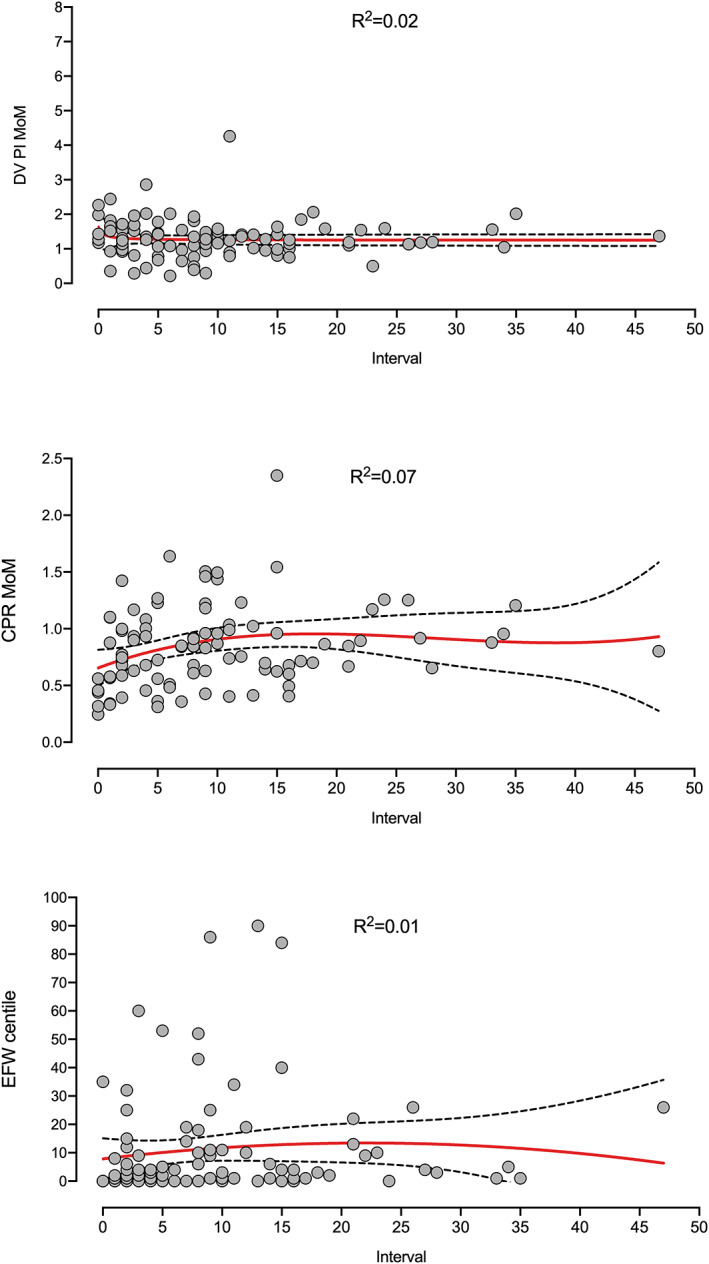
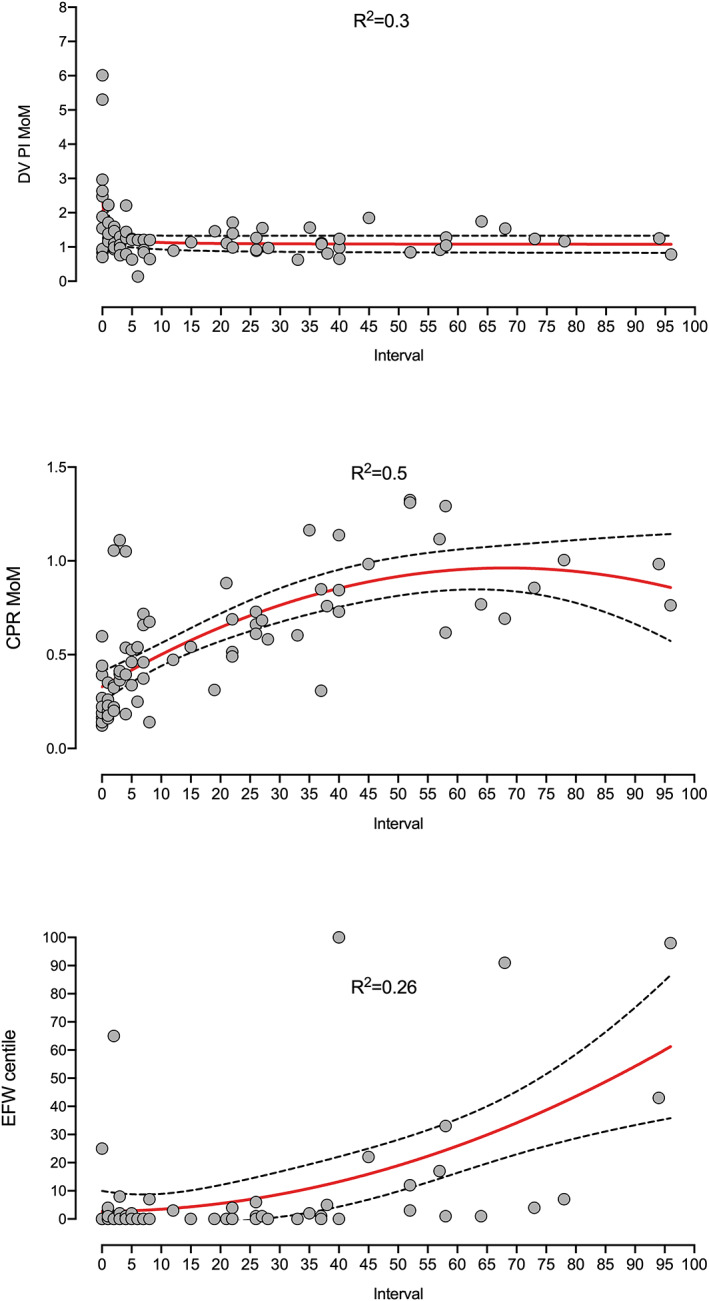
Material and methods: This was a retrospective study of 169 high-risk pregnancies (72 < 34 and 97 ≥ 34 weeks) that underwent an ultrasound examination of CPR, DV Doppler and estimated fetal weight at 22-40 weeks. The CPR and DV PI were converted into multiples of the median, and the estimated fetal weight into centiles according to local references. Adverse perinatal outcome was defined as a composite of abnormal cardiotocogram, intrapartum pH requiring cesarean delivery, 5' Apgar score <7, neonatal pH <7.10 and admission to neonatal intensive care unit. Values were plotted according to the interval to labor to evaluate progression of abnormal Doppler values, and their accuracy was evaluated at both gestational periods, alone and combined with clinical data, by means of univariable and multivariable models, using the Akaike information criteria (AIC) and the area under the curve (AUC).
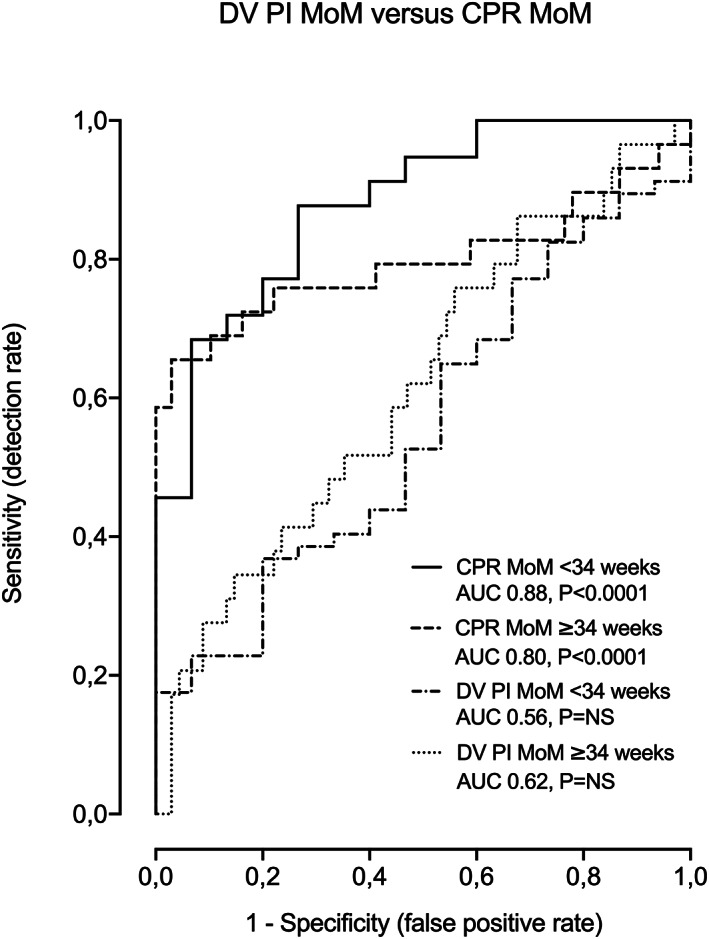
Results: Prior to 34 weeks' gestation, DV PI was the latest parameter to become abnormal. However, it was a poor predictor of adverse perinatal outcome (AUC 0.56, 95% CI: 0.40-0.71, AIC 76.2, p > 0.05), and did not improve the predictive accuracy of CPR for adverse perinatal outcome (AUC 0.88, 95% CI: 0.79-0.97, AIC 52.9, p < 0.0001). After 34 weeks' gestation, the chronology of the DV PI and CPR anomalies overlapped, but again DV PI was a poor predictor for adverse perinatal outcome (AUC 0.62, 95% CI: 0.49-0.74, AIC 120.6, p > 0.05), that did not improve the CPR ability to predict adverse perinatal outcome (AUC 0.80, 95% CI: 0.67-0.92, AIC 106.8, p < 0.0001). The predictive accuracy of CPR prior to 34 weeks persisted when the gestational age at delivery was included in the model (AUC 0.91, 95% CI: 0.81-1.00, AIC 46.3, p < 0.0001, vs AUC 0.86, 95% CI: 0.72-1, AIC 56.1, p < 0.0001), and therefore was not determined by prematurity.
Conclusions: CPR predicts adverse perinatal outcome better than DV PI, regardless of gestational age. Larger prospective studies are needed to delineate the role of ultrasound tools of fetal wellbeing assessment in predicting and preventing adverse perinatal outcome.
Keywords: adverse perinatal outcome; cerebroplacental ratio; ductus venosus Doppler; fetal Doppler.
© 2023 The Authors. Acta Obstetricia et Gynecologica Scandinavica published by John Wiley & Sons Ltd on behalf of Nordic Federation of Societies of Obstetrics and Gynecology (NFOG).
Conflict of interest statement
The authors report no conflict of interests.
Figures
Similar articles
-
Routine assessment of cerebroplacental ratio at 35-37 weeks' gestation in the prediction of adverse perinatal outcome.Am J Obstet Gynecol. 2019 Jul;221(1):65.e1-65.e18. doi: 10.1016/j.ajog.2019.03.002. Epub 2019 Mar 13. Am J Obstet Gynecol. 2019. PMID: 30878322
-
Role of Doppler ultrasound at time of diagnosis of late-onset fetal growth restriction in predicting adverse perinatal outcome: prospective cohort study.Ultrasound Obstet Gynecol. 2020 Jun;55(6):793-798. doi: 10.1002/uog.20406. Epub 2020 May 8. Ultrasound Obstet Gynecol. 2020. PMID: 31343783
-
Prediction of adverse perinatal outcome by cerebroplacental ratio in women undergoing induction of labor.Ultrasound Obstet Gynecol. 2019 Apr;53(4):473-480. doi: 10.1002/uog.20173. Epub 2019 Mar 4. Ultrasound Obstet Gynecol. 2019. PMID: 30426578
-
Comparison between cerebroplacental ratio and umbilicocerebral ratio in predicting adverse perinatal outcome at term.Eur J Obstet Gynecol Reprod Biol. 2020 Sep;252:439-443. doi: 10.1016/j.ejogrb.2020.07.032. Epub 2020 Jul 24. Eur J Obstet Gynecol Reprod Biol. 2020. PMID: 32763648 Review.
-
Role of umbilicocerebral and cerebroplacental ratios in prediction of perinatal outcome in FGR pregnancies.Arch Gynecol Obstet. 2022 Jun;305(6):1383-1392. doi: 10.1007/s00404-021-06268-4. Epub 2021 Oct 2. Arch Gynecol Obstet. 2022. PMID: 34599678 Free PMC article. Review.
Cited by
-
Diagnostic value of combined maternal cardiac work and fetoplacental circulation parameters in detecting fetal intrauterine hypoxia in preeclamptic women.Sci Rep. 2024 Dec 28;14(1):31209. doi: 10.1038/s41598-024-82545-x. Sci Rep. 2024. PMID: 39732899 Free PMC article.
References
-
- Figueras F, Gratacós E. Update on the diagnosis and classification of fetal growth restriction and proposal of a stage‐based management protocol. Fetal Diagn Ther. 2014;36:86‐98. - PubMed
-
- Figueras F, Caradeux J, Crispi F, Eixarch E, Peguero A, Gratacos E. Diagnosis and surveillance of late‐onset fetal growth restriction. Am J Obstet Gynecol. 2018;218:S790‐S802.e1. - PubMed
-
- Figueras F, Gratacos E. An integrated approach to fetal growth restriction. Best Pract Res Clin Obstet Gynaecol. 2017;38:48‐58. - PubMed
-
- Bligh LN, Al Solai A, Greer RM, Kumar S. Diagnostic performance of cerebroplacental ratio thresholds at term for prediction of low birthweight and adverse intrapartum and neonatal outcomes in a term. Low‐Risk Population Fetal Diagn Ther. 2018;43:191‐198. - PubMed
-
- Bligh LN, Alsolai AA, Greer RM, Kumar S. Cerebroplacental ratio thresholds measured within 2 weeks before birth and risk of cesarean section for intrapartum fetal compromise and adverse neonatal outcome. Ultrasound Obstet Gynecol. 2018;52:340‐346. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
