

Long-Term High Flow Nasal Cannula Therapy in Primary and Secondary Bronchiectasis
- PMID: 37174791
- PMCID: PMC10178516
- DOI: 10.3390/healthcare11091250
Long-Term High Flow Nasal Cannula Therapy in Primary and Secondary Bronchiectasis
Abstract
Background: Bronchiectasis is the consequence of chronic bronchial inflammation, inappropriate mucus clearance, bacterial colonization, and recurrent or chronic infection. High flow therapy (HFT) is a type of non-invasive respiratory therapy, usually delivered through a nasal cannula interface (HFNC). It delivers heated and humidified air with a stable fraction of inspired oxygen and a wide range of possible flow rates.
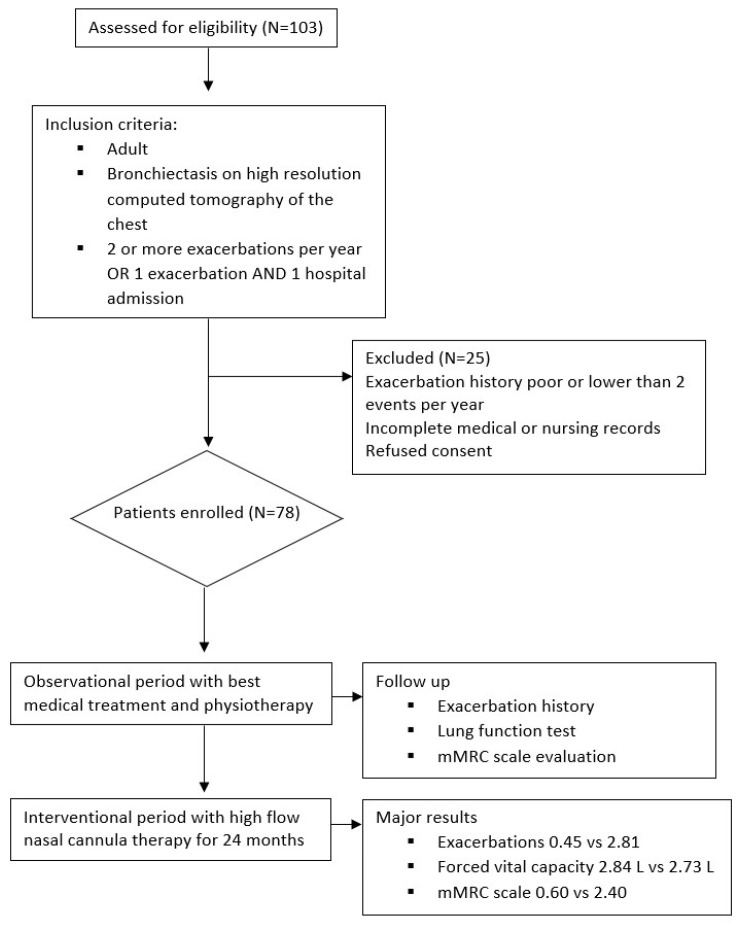
Aim of the study: Determine the effectiveness of HFNC as add-on therapy in adult primary and secondary bronchiectasis with frequent acute exacerbations (AEs) and/or hospitalizations.
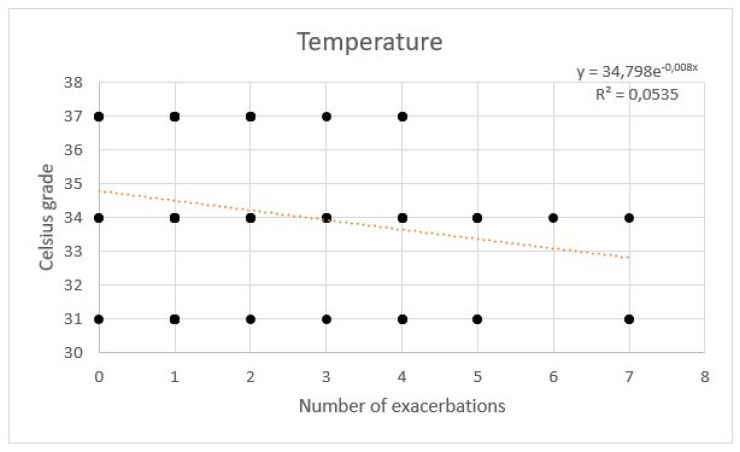
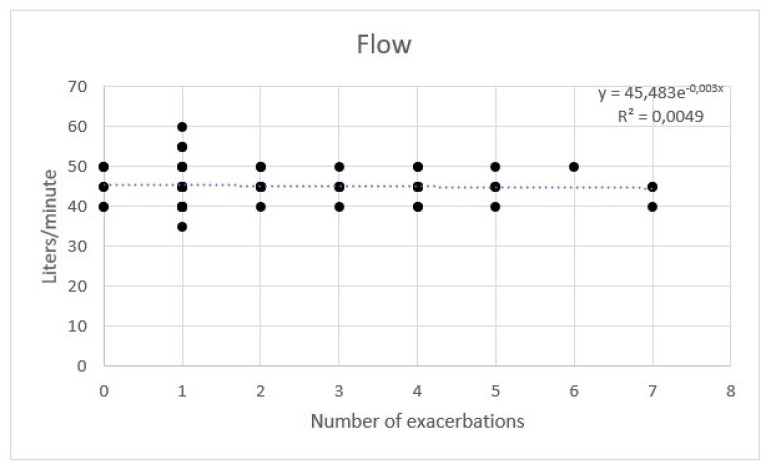
Methods: This is a single-center crossover study on long-term home therapy with HFNC in adult bronchiectasis. Pharmacological therapy included pulse therapy with mucolytics and bronchodilators. After one year, all patients were switched to additional HFNC. The temperature range was 31-37 °C. The flow range was 35-60 L/m. FiO2 was 0.21.
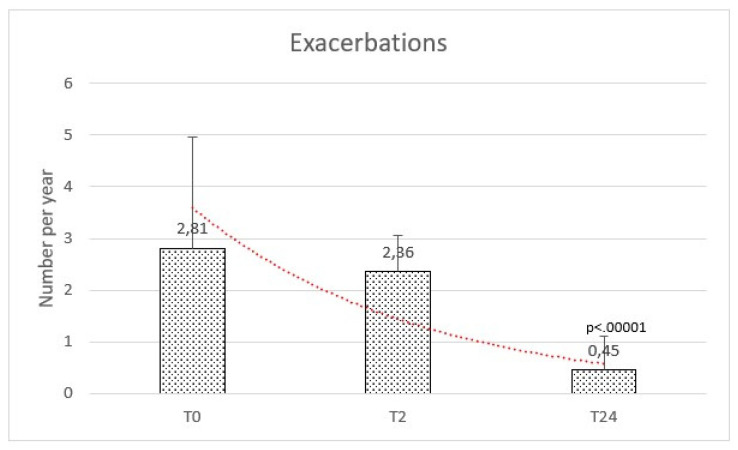
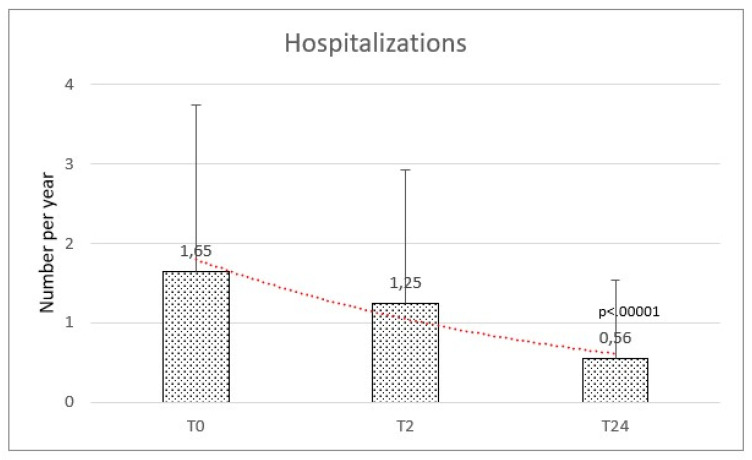
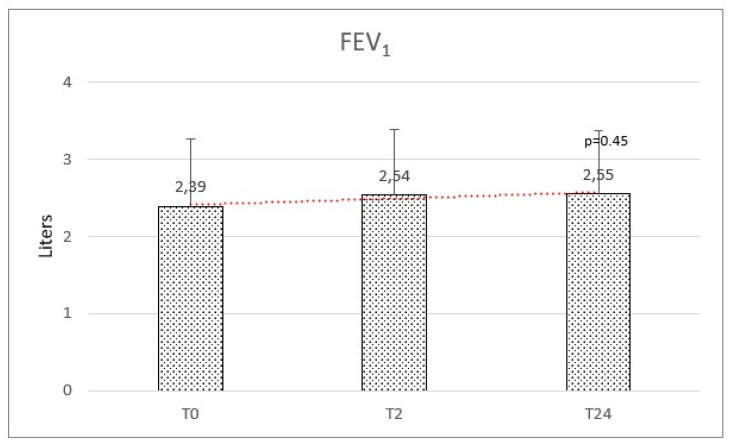
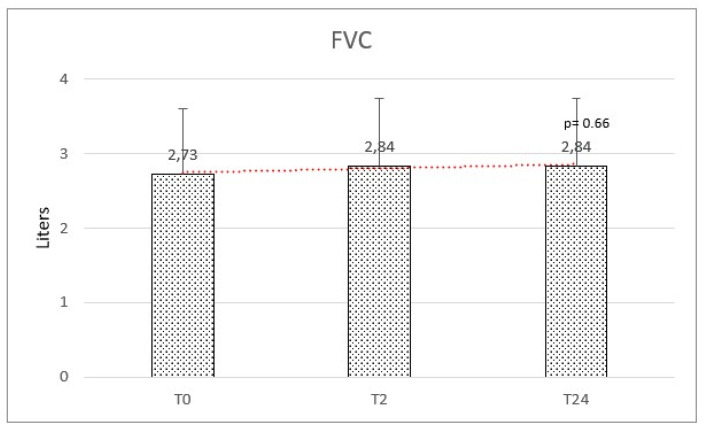
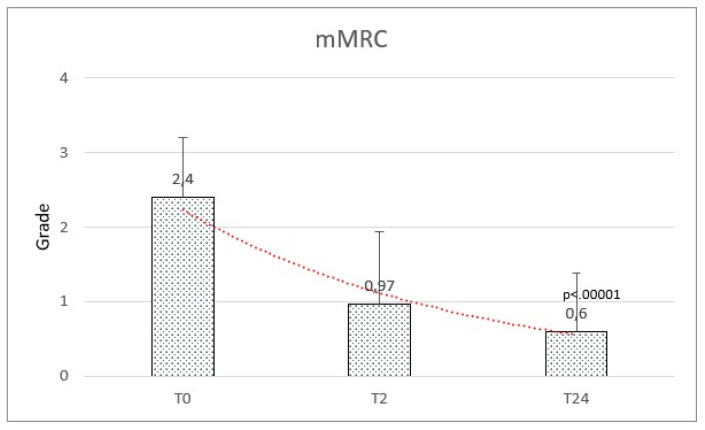
Results: Seventy-eight patients completed the follow-up; 54% were females; the median age was 70 years (IQR 60-76). The etiology of bronchiectasis was mainly post-infective (51%), COPD related (26%), and congenital (11%). AEs at baseline were 2.81 (±2.15). A significant reduction in AEs was observed after 24 months with a mean of 0.45 (±0.66) (f-ratio value 79.703. p-value < 0.00001). No significant difference was observed after HFNC therapy on FEV1 (2.39 ± 0.87 vs. 2.55 ± 0.82; f-ratio 0.79. p-value 0.45) and FVC (2.73 ± 0.88 vs. 2.84 ± 0.90; f-ratio 0.411. p-value 0.66). A significant reduction in mMRC score was observed after HFNC therapy (2.40 ± 0.81 vs. 0.97 ± 0.97 at 2 months vs. 0.60 ± 0.78 at 24 months; f-ratio value 95.512. p-value < 0.00001).
Conclusions: HFNC is a well-tolerated add-on therapy for adult bronchiectasis. Dyspnea improved after 2 months and further after 2 years. The exacerbation rate decreased during the 2 years follow-up. No significant difference was observed in lung function.
Keywords: COPD; cystic fibrosis; heated and humidified therapy; mucus; rehabilitation.
Conflict of interest statement
No competing interest to declare.
Figures
References
-
- Cole P.J. Inflammation: A two-edged sword—The model of bronchiectasis. Eur. J. Respir. Dis. Suppl. 1986;147:6–15. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
