

Pulmonary Hypertension in Chronic Lung Diseases: What Role Do Radiologists Play?
- PMID: 37174998
- PMCID: PMC10178805
- DOI: 10.3390/diagnostics13091607
Pulmonary Hypertension in Chronic Lung Diseases: What Role Do Radiologists Play?
Abstract
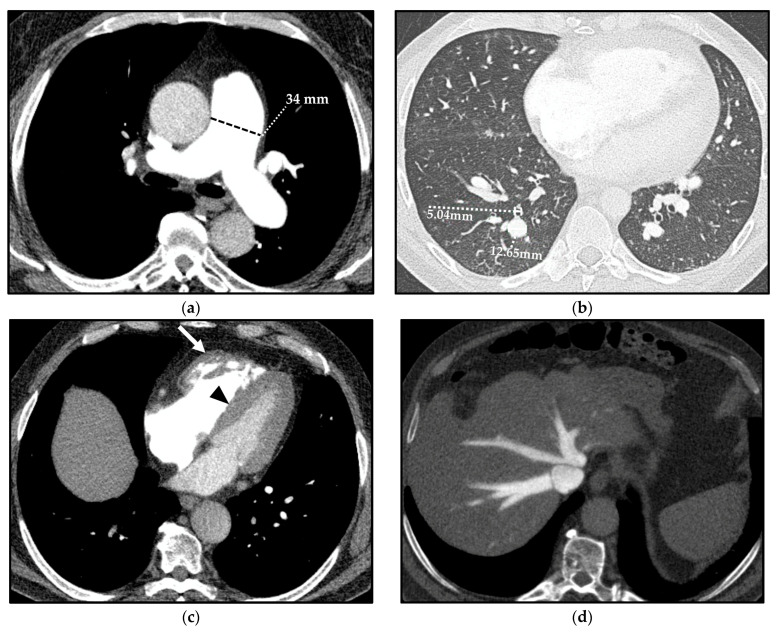
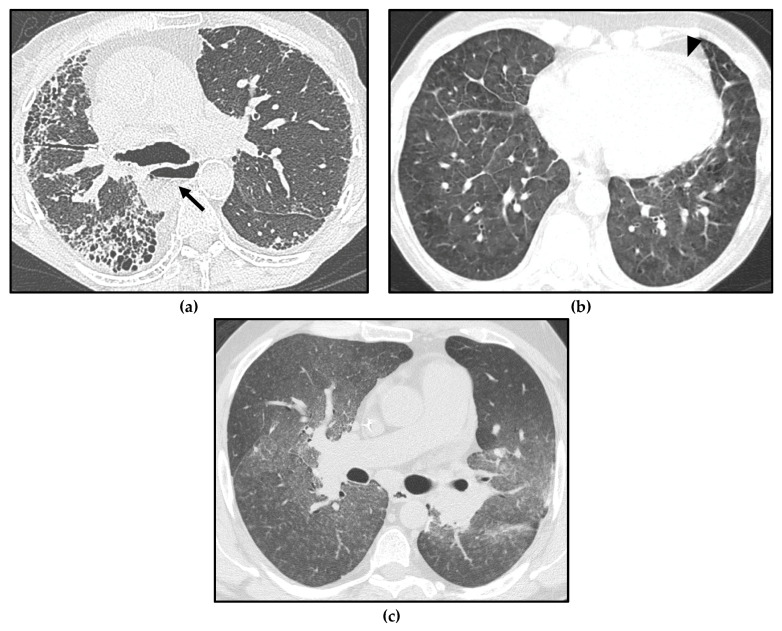
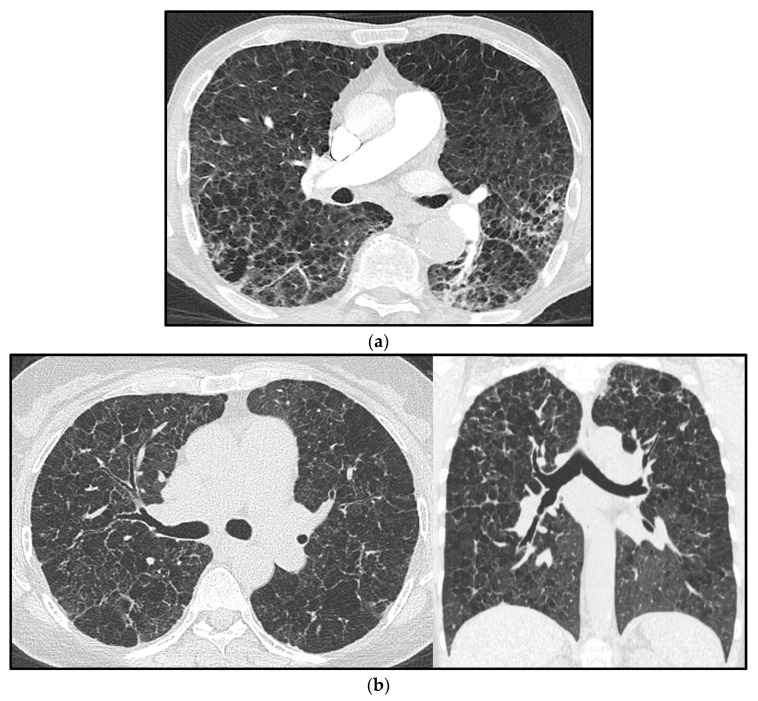
Pulmonary hypertension (PH) is a pathophysiological disorder, defined by a mean pulmonary arterial pressure (mPAP) > 20 mmHg at rest, as assessed by right heart catheterization (RHC). PH is not a specific disease, as it may be observed in multiple clinical conditions and may complicate a variety of thoracic diseases. Conditions associated with the risk of developing PH are categorized into five different groups, according to similar clinical presentations, pathological findings, hemodynamic characteristics, and treatment strategy. Most chronic lung diseases that may be complicated by PH belong to group 3 (interstitial lung diseases, chronic obstructive pulmonary disease, combined pulmonary fibrosis, and emphysema) and are associated with the lowest overall survival among all groups. However, some of the chronic pulmonary diseases may develop PH with unclear/multifactorial mechanisms and are included in group 5 PH (sarcoidosis, pulmonary Langerhans' cell histiocytosis, and neurofibromatosis type 1). This paper focuses on PH associated with chronic lung diseases, in which radiological imaging-particularly computed tomography (CT)-plays a crucial role in diagnosis and classification. Radiologists should become familiar with the hemodynamical, physiological, and radiological aspects of PH and chronic lung diseases in patients at risk of developing PH, whose prognosis and treatment depend on the underlying disease.
Keywords: chronic lung diseases; computed tomography; imaging; pulmonary hypertension.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Humbert M., Kovacs G., Hoeper M.M., Badagliacca R., Berger R.M.F., Brida M., Carlsen J., Coats A.J.S., Escribano-Subias P., Ferrari P., et al. ESC/ERS Scientific Document Group 2022 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension. Eur. Heart J. 2022;43:3618–3731. doi: 10.1093/eurheartj/ehac237. - DOI - PubMed
-
- Remy-Jardin M., Ryerson C.J., Schiebler M.L., Leung A.N.C., Wild J.M., Hoeper M.M., Alderson P.O., Goodman L.R., Mayo J., Haramati L.B., et al. Imaging of pulmonary hypertension in adults: A position paper from the Fleischner Society. Eur. Respir. J. 2021;57:2004455. doi: 10.1183/13993003.04455-2020. - DOI - PubMed
-
- Maron B.A., Hess E., Maddox T.M., Opotowsky A.R., Tedford R.J., Lahm T., Joynt K.E., Kass D.J., Stephens T., Stanislawski M.A., et al. Association of borderline pulmonary hypertension with mortality and hospitalization in a large patient cohort: Insights from the veterans affairs clinical assessment, reporting, and tracking program. Circulation. 2016;133:1240–1248. doi: 10.1161/CIRCULATIONAHA.115.020207. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
