

Diagnosis of Laryngopharyngeal Reflux: Past, Present, and Future-A Mini-Review
- PMID: 37175034
- PMCID: PMC10177910
- DOI: 10.3390/diagnostics13091643
Diagnosis of Laryngopharyngeal Reflux: Past, Present, and Future-A Mini-Review
Abstract
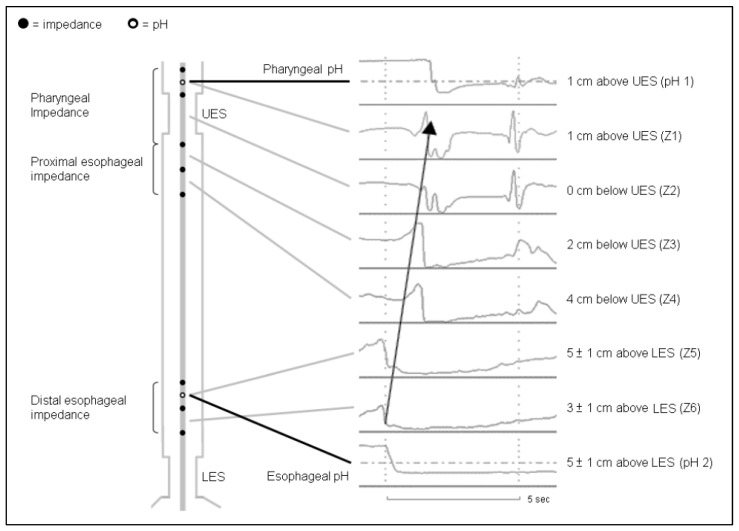
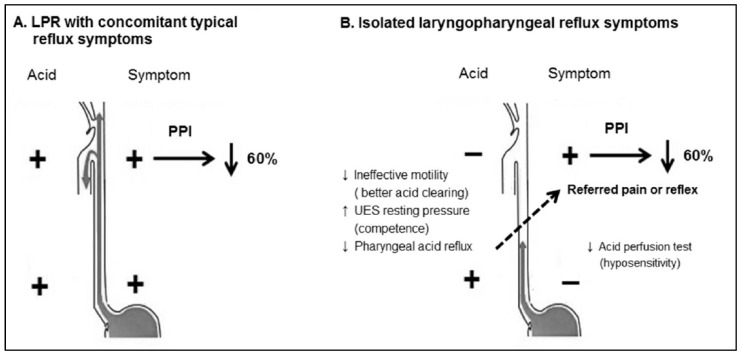
Laryngopharyngeal reflux (LPR) is a variant of gastroesophageal reflux disease (GERD) in which gastric refluxate irritates the lining of the aerodigestive tract and causes troublesome airway symptoms or complications. LPR is a prevalent disease that creates a significant socioeconomic burden due to its negative impact on quality of life, tremendous medical expense, and possible cancer risk. Although treatment modalities are similar between LPR and GERD, the diagnosis of LPR is more challenging than GERD due to its non-specific symptoms/signs. Due to the lack of pathognomonic features of endoscopy, mounting evidence focused on physiological diagnostic testing. Two decades ago, a dual pH probe was considered the gold standard for detecting pharyngeal acidic reflux episodes. Despite an association with LPR, the dual pH was unable to predict the treatment response in clinical practice, presumably due to frequently encountered artifacts. Currently, hypopharygneal multichannel intraluminal impedance-pH catheters incorporating two trans-upper esophageal sphincter impedance sensors enable to differentiate pharyngeal refluxes from swallows. The validation of pharyngeal acid reflux episodes that are relevant to anti-reflux treatment is, therefore, crucial. Given no diagnostic gold standard of LPR, this review article aimed to discuss the evolution of objective diagnostic testing and its predictive role of treatment response.
Keywords: hypopharyngeal multichannel intraluminal impedance-pH; laryngopharyngeal reflux; pharyngeal acid reflux episodes.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
How many cases of laryngopharyngeal reflux suspected by laryngoscopy are gastroesophageal reflux disease-related?World J Gastroenterol. 2012 Aug 28;18(32):4363-70. doi: 10.3748/wjg.v18.i32.4363. World J Gastroenterol. 2012. PMID: 22969200 Free PMC article.
-
Symptoms classically attributed to laryngopharyngeal reflux correlate poorly with pharyngeal reflux events on multichannel intraluminal impedance testing.Dis Esophagus. 2022 Dec 31;36(1):doac041. doi: 10.1093/dote/doac041. Dis Esophagus. 2022. PMID: 35780323
-
Dual pH Probes Without Proximal Esophageal and Pharyngeal Impedance May Be Deficient in Diagnosing LPR.J Voice. 2019 Sep;33(5):697-703. doi: 10.1016/j.jvoice.2018.03.008. Epub 2018 Aug 3. J Voice. 2019. PMID: 30082108
-
Evaluation and management of laryngopharyngeal reflux.JAMA. 2005 Sep 28;294(12):1534-40. doi: 10.1001/jama.294.12.1534. JAMA. 2005. PMID: 16189367 Review.
-
Diagnostic Testing for Laryngopharyngeal Reflux Disease: The Role of 24-hour Hypopharyngeal-Esophageal Multichannel Intraluminal Impedance-pH Monitoring.Otolaryngol Clin North Am. 2025 Jun;58(3):441-449. doi: 10.1016/j.otc.2024.12.001. Epub 2025 Jan 7. Otolaryngol Clin North Am. 2025. PMID: 39779436 Review.
Cited by
-
Diagnostic Value of Fasting and Bedtime Saliva Pepsin Measurements in Laryngopharyngeal Reflux.Biomedicines. 2024 Feb 8;12(2):398. doi: 10.3390/biomedicines12020398. Biomedicines. 2024. PMID: 38398000 Free PMC article.
-
Is empiric proton pump inhibition in patients with symptoms of extraesophageal gastroesophageal reflux justified?BMC Gastroenterol. 2023 Sep 6;23(1):303. doi: 10.1186/s12876-023-02945-7. BMC Gastroenterol. 2023. PMID: 37674110 Free PMC article. Review.
-
Reflux Testing: Wireless pH, Impedance-pH, and Mucosal Impedance.Gastrointest Endosc Clin N Am. 2025 Jul;35(3):587-601. doi: 10.1016/j.giec.2024.12.007. Epub 2025 Jan 23. Gastrointest Endosc Clin N Am. 2025. PMID: 40412992 Review.
-
Evaluating the long-term efficacy of robotic anti-reflux surgery on symptom resolution in gerd patients: a comprehensive analysis of typical and atypical presentations.Surg Endosc. 2025 Aug 14. doi: 10.1007/s00464-025-11975-z. Online ahead of print. Surg Endosc. 2025. PMID: 40813906
-
Accuracy of COuGH RefluX Score as a Predictor of Gastroesophageal Reflux Disease (GERD) in Mexican Patients with Chronic Laryngopharyngeal Symptoms: A Cross-Sectional Study.Diagnostics (Basel). 2025 Mar 6;15(5):636. doi: 10.3390/diagnostics15050636. Diagnostics (Basel). 2025. PMID: 40075882 Free PMC article.
References
-
- Koufman J.A., Aviv J.E., Casiano R.R., Shaw G.Y. Laryngopharyngeal reflux: Position statement of the committee on speech, voice, and swallowing disorders of the American Academy of Otolaryngology-Head and Neck Surgery. Otolaryngol. Head Neck Surg. 2002;127:32–35. doi: 10.1067/mhn.2002.125760. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
