

Imaging of ovarian lymphoma
- PMID: 37178392
- PMCID: PMC10632316
- DOI: 10.1007/s40477-023-00779-3
Imaging of ovarian lymphoma
Erratum in
-
Correction to: Imaging of ovarian lymphoma.J Ultrasound. 2023 Dec;26(4):959. doi: 10.1007/s40477-023-00799-z. J Ultrasound. 2023. PMID: 37269426 Free PMC article. No abstract available.
Abstract
Objective: The aim of the study is to describe the radiological spectrum of appearances of ovarian lymphoma (OL). The manuscript describes the radiological aspects of OL to assist the radiologist in achieving correct orientation of the diagnosis.
Methods: We conducted a retrospective evaluation of imaging studies of 98 cases of non-Hodgkin's lymphoma, with extra-nodal localisation (ovaries) in three cases (1 primary, 2 secondary). A literature review was also performed.
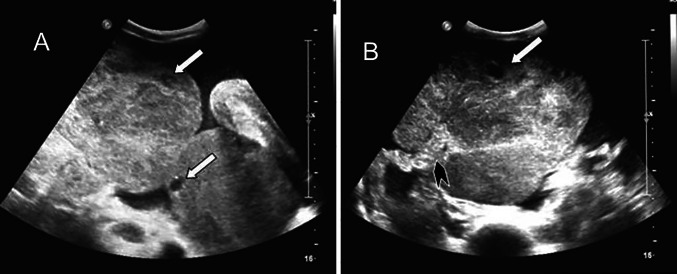
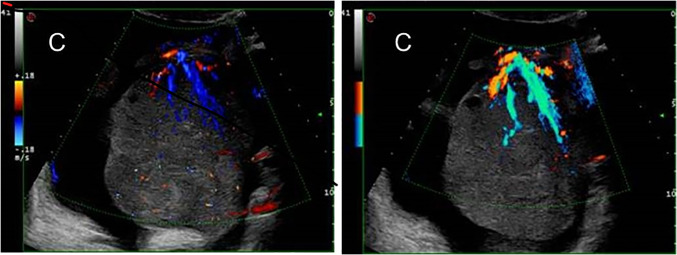
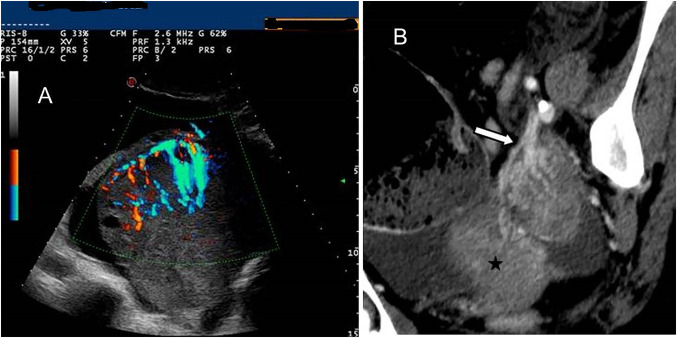
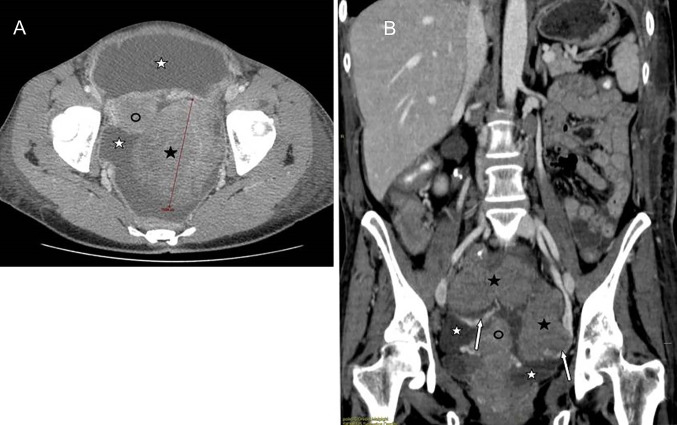
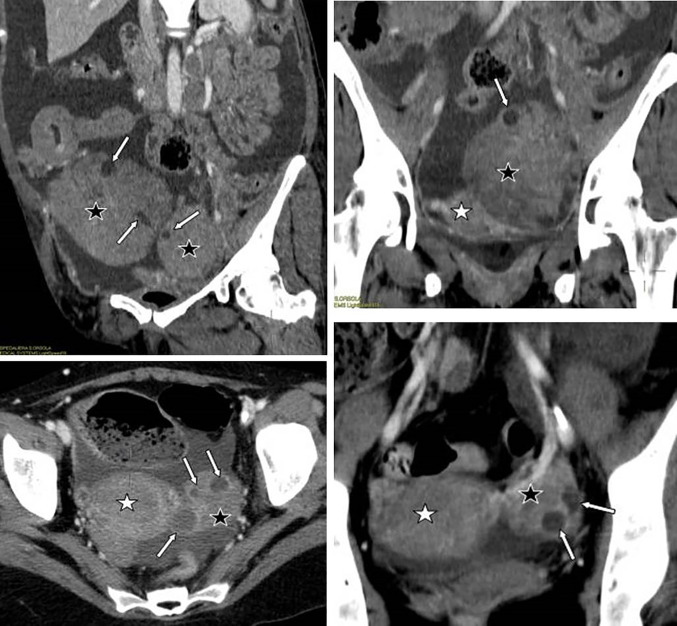
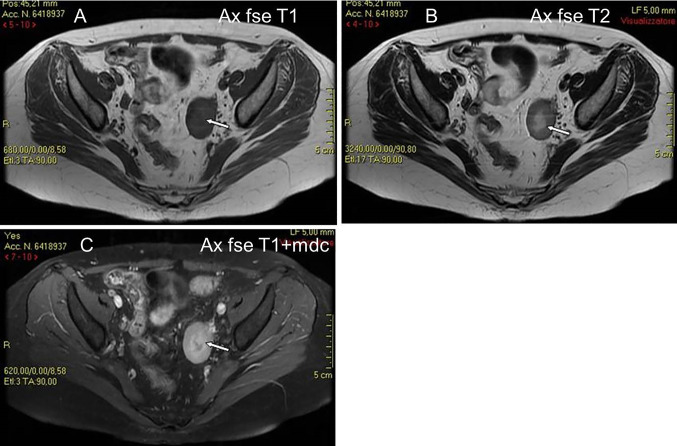
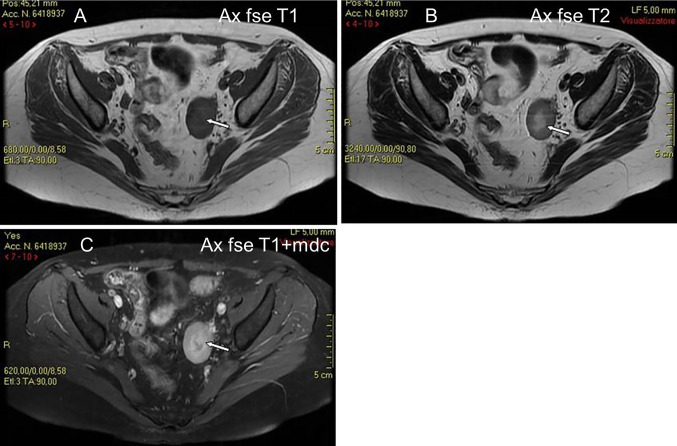
Results: Of the three evaluated women, one had a primary ovarian involvement and two had a secondary ovarian involvement. The most common lesion characteristics were a well-defined, solid homogeneous and hypoechoic mass at US. CT depicts OL as a well-defined, non-infiltrating, homogeneous hypodense solid mass, with mild contrast enhancement. On T1-weight MRI, OL appears as a homogeneous mass of low signal intensity, which enhances avidly following intravenous gadolinium.
Conclusion: Clinical and serological presentation of OL can be similar to that of primary ovarian cancer. As imaging plays a central role in the diagnosis of OL, the radiologist should be familiar with US, CT and MRI appearances of this condition to correctly orient the diagnosis and so avoid unnecessary adnexectomy.
Keywords: Lead vessel; Lymphoma; Ovarian lymphoma; Ovarian neoplasms.
© 2023. Società Italiana di Ultrasonologia in Medicina e Biologia (SIUMB).
Conflict of interest statement
The authors have not disclosed any competing interests.
Figures
References
-
- Ferry JA, Young RH. Malignant lymphoma, pseudolymphoma and hemopoeitic disorders of the female genital tract. Pathol Annu. 1991;26:227–263. - PubMed
-
- Yun J, Kim SJ, Won JH, Choi CW, Eom HS, Kim JS, Kim MK, Kwak J, Suh WSK. Clinical features and prognostic relevance of ovarian involvement in non-Hodgkin's lymphoma: a consortium for improving survival of lymphoma (CISL) report. Leuk Res. 2010;34:1175–1179. doi: 10.1016/j.leukres.2010.02.010. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
