

The impact of recommending iron supplements to women with depleted iron stores in early pregnancy on use of supplements, and factors associated with changes in iron status from early pregnancy to postpartum in a multi-ethnic population-based cohort
- PMID: 37179290
- PMCID: PMC10182636
- DOI: 10.1186/s12884-023-05668-5
The impact of recommending iron supplements to women with depleted iron stores in early pregnancy on use of supplements, and factors associated with changes in iron status from early pregnancy to postpartum in a multi-ethnic population-based cohort
Abstract
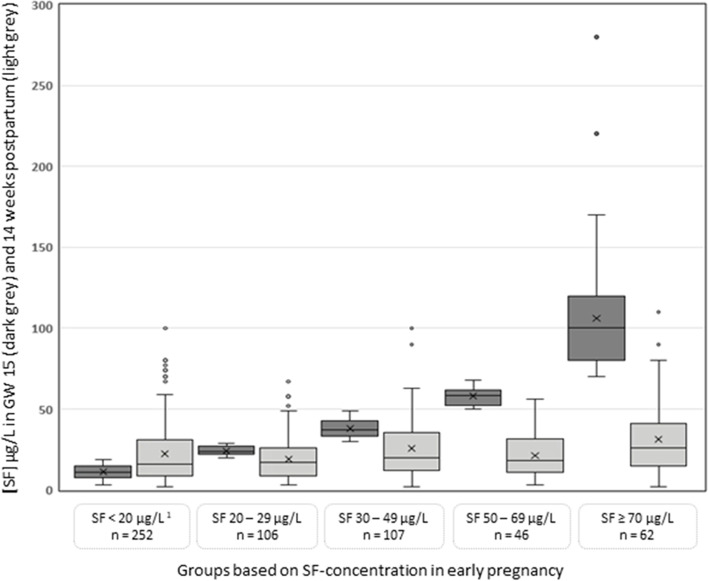
Background: We aimed to evaluate the impact of recommending supplementation to pregnant women with serum ferritin (SF) < 20 µg/L in early pregnancy on use of supplements, and to explore which factors were associated with changes in iron status by different iron indicators to 14 weeks postpartum.
Methods: A multi-ethnic population-based cohort study of 573 pregnant women examined at mean gestational week (GW) 15 (enrolment), at mean GW 28 and at the postpartum visit (mean 14 weeks after delivery). Women with SF < 20 µg/L at enrolment were recommended 30-50 mg iron supplementation and supplement use was assessed at all visits. Change of SF, soluble transferrin receptor and total body iron from enrolment to postpartum were calculated by subtracting the concentrations at the postpartum visit from that at enrolment. Linear and logistic regression analyses were performed to assess associations between use of supplements in GW 28 and changes in iron status and postpartum iron deficiency/anaemia. Change of iron status was categorized into 'steady low', 'improvement', 'deterioration', and 'steady high' based on SF status at enrolment and postpartum. Multinomial logistic regression analyses were performed to identify factors associated with change of iron status.
Results: At enrolment, 44% had SF < 20 µg/L. Among these women (78% non-Western European origin), use of supplements increased from 25% (enrolment) to 65% (GW 28). Use of supplements in GW 28 was associated with improved iron levels by all three indicators (p < 0.05) and with haemoglobin concentration (p < 0.001) from enrolment to postpartum, and with lower odds of postpartum iron deficiency by SF and TBI (p < 0.05). Factors positively associated with 'steady low' were: use of supplements, postpartum haemorrhage, an unhealthy dietary pattern and South Asian ethnicity (p ≤ 0.01 for all); with 'deterioration': postpartum haemorrhage, an unhealthy dietary pattern, primiparity and no use of supplements (p < 0.01 for all), and with 'improvement': use of supplements, multiparity and South Asian ethnicity (p < 0.03 for all).
Conclusions: Both supplement use and iron status improved from enrolment to the postpartum visit among women recommended supplementation. Dietary pattern, use of supplements, ethnicity, parity and postpartum haemorrhage were identified as factors associated with change in iron status.
Keywords: Anaemia; Ethnic minority; Iron deficiency; Maternal and Child health; Nutrition; Pregnancy; Supplementation.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Nutritional anaemias: tools for effective prevention and control. Geneva: World Health Organization; 2017.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
