

The inferior alveolar nerve at the proximal fragment during bilateral sagittal split osteotomy - Is there need to reposition to distal fragment?
- PMID: 37179846
- PMCID: PMC10173002
- DOI: 10.1016/j.jobcr.2023.04.001
The inferior alveolar nerve at the proximal fragment during bilateral sagittal split osteotomy - Is there need to reposition to distal fragment?
Erratum in
-
Erratum regarding missing declaration of competing interest statements in previously published articles.J Oral Biol Craniofac Res. 2024 Jul-Aug;14(4):360-361. doi: 10.1016/j.jobcr.2024.05.009. Epub 2024 May 23. J Oral Biol Craniofac Res. 2024. PMID: 38826841 Free PMC article.
Abstract
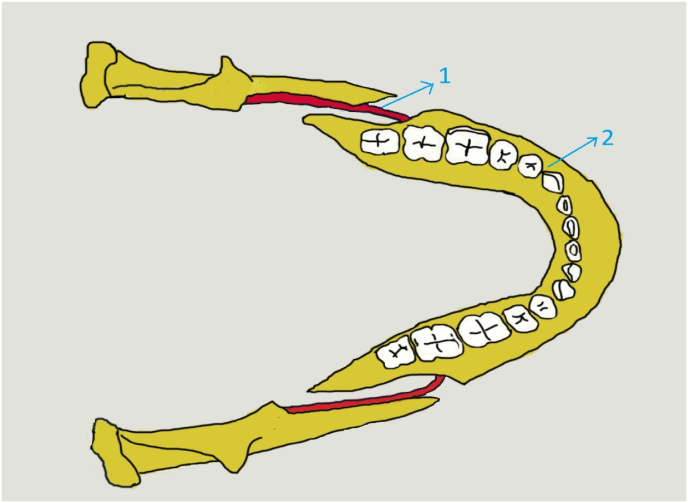
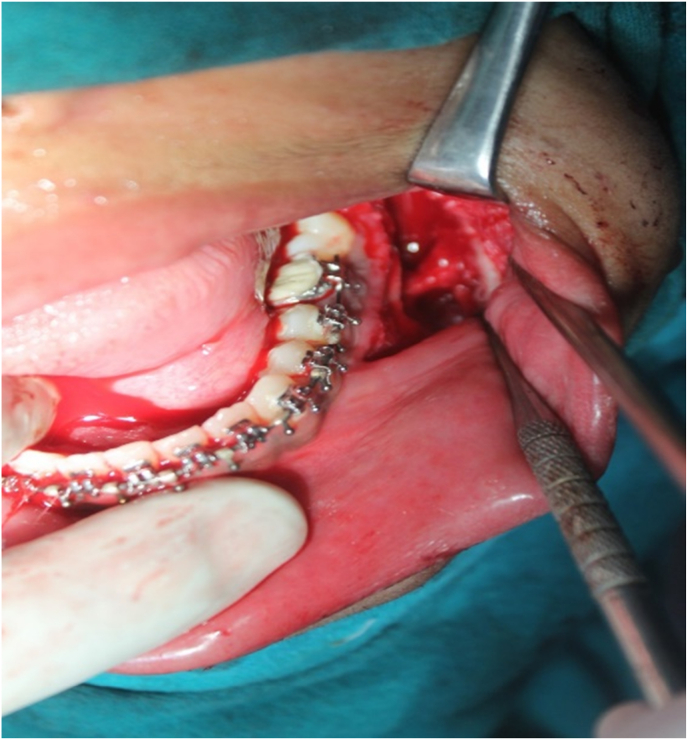
Inferior alveolar nerve (IAN) injury is most common in bilateral sagittal split osteotomy (BSSO) cases. The present standard is to always reposition the IAN from the proximal fragment to the distal fragment during surgery. This study aims to assess the severity and incidence of postoperative injury and the recovery of the inferior alveolar nerve in proximal fragment entrapment.
Methods: - A total of 35 patients (70 BSSO osteotomies) with mandibular deformities requiring movements equal to or less than 6 mm were selected. Twenty out of 70 osteotomies had IAN on the proximal fragment (Group 1) while splitting. Group 2 included 20 osteotomies with IAN on the distal segment in the same patients. Therefore, 15 patients who had IAN on distal segments on both sides were excluded from this study. All the BSSO procedures were performed by the same surgeon. Postoperative recovery and follow-up were performed on the immediate 1st postoperative day and at 3-, 6- and 12-month intervals. The nociception (pin-prick discrimination) test and mechanoreceptive tactile skin test with cotton fibrils were performed by a third clinician who was blinded to the procedure to assess IAN sensation.
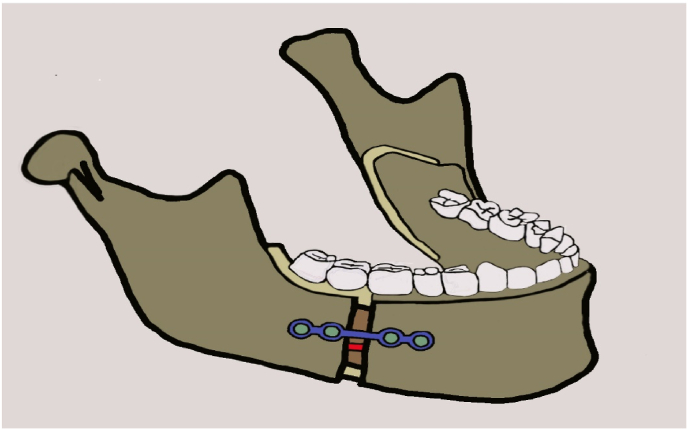
Conclusion: There was no significant difference between the groups in the recovery of IAN sensation after 6 months and the 1-year period. Hence reposition of IAN from the proximal segment to the distal segment during BSSO surgery may not be mandatory if the required movement is within 6 mm. This avoids unnecessary manipulation of the IAN over the proximal fragment.
Keywords: BSSO; BSSO complications; IAN recovery; Inferior alveolar nerve injury.
© 2023 The Author(s).
Figures




References
-
- Agbaje J.O., Salem A.S., Lambrichts I., Jacobs R., Politis C. Systematic review of the incidence of inferior alveolar nerve injury in bilateral sagittal split osteotomy and the assessment of neurosensory disturbances. Int J Oral Maxillofac Surg. 2015;44:447–451. - PubMed
-
- Tabrizi R., Behnia H., Behnia P., Ozkan B.T. What factors affect the attachment of the inferior alveolar nerve to the buccal plate following sagittal split osteotomy? J Cranio-Maxillofacial Surg. 2020;48(5):483–487. - PubMed
-
- Politis C., Lambrichts I., Sun Y., Vrielinck L., Schepers S., Agbaje JO lubanw Attachment rate of the inferior alveolar nerve to buccal plate during bilateral sagittal split osteotomy influences self-reported sensory impairment. J Craniofac Surg. 2014;25(6):2121–2126. - PubMed
-
- Panula K., Finne K., Oikarinen K. Neurosensory deficits after bilateral sagittal split ramus osteotomy of the mandible - influence of soft tissue handling medial to the ascending ramus. Int J Oral Maxillofac Surg. 2004;33(6):543–548. - PubMed
-
- Kuhlefelt M., Laine P., Suominen A.L., Lindqvist C., Thorén H. Nerve manipulation during bilateral sagittal split osteotomy increases neurosensory disturbance and decreases patient satisfaction. J Oral Maxillofac Surg. 2014;72(10):2052.e1–2052.e5. - PubMed
LinkOut - more resources
Full Text Sources
