

'Granulomatosis with polyangiitis after Pfizer vaccination': a case report
- PMID: 37180416
- PMCID: PMC10032451
- DOI: 10.1177/26330040221130084
'Granulomatosis with polyangiitis after Pfizer vaccination': a case report
Abstract
The advent of COVID-19, caused by the SARS-CoV-2 virus, has resulted in over 541 million cases with 6.32 million deaths worldwide as of June 2022. The devastating consequences of this global pandemic resulted in the expedited generation of mRNA-based vaccines such as the Pfizer-BioNTech and Moderna vaccines. Although the vaccines have been effective, with recent data indicating greater than 95% effectiveness, rare complications have been reported, including manifestations of autoimmune phenomena. Herein, we report a rare case of Granulomatosis with polyangiitis (GPA) in an active duty military male soon after receiving the first dose of the Pfizer-BioNTech COVID-19 vaccine.
Keywords: ANCA vasculitis; COVID-19 Pfizer vaccine; granulomatous with polyangiitis; hemoptysis; pauci-immune glomerulonephritis.
Plain language summary
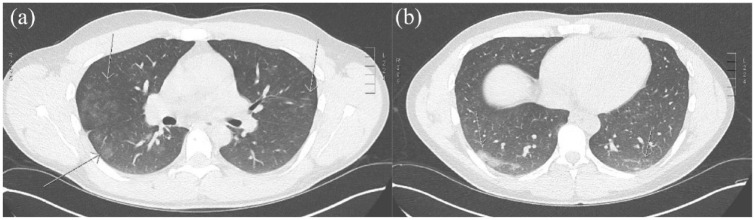
A 27-year-old active duty marine was admitted to our hospital after being transferred from Hawaii with concern of new autoimmune disease after receiving the Pfizer vaccine. The patient initially presented to the emergency department with joint pain, fever, chest pain, hemoptysis, and a nose bleed. A comprehensive workup demonstrated elevated inflammatory markers, progressive renal dysfunction, and a positive antibody panel consistent with antineutrophil cytoplasmic antibodies (ANCA) vasculitis. Due to the limited capabilities in his deployed setting, he was transferred to our hospital for a higher level of care. We performed some additional tests to include computed tomography (CT) imaging of his lungs and a renal biopsy which came back consistent with GPA. The patient was started on high-dose prednisone and rituximab, and he achieved remission. He was discharged from the hospital with follow-up arranged with rheumatology and nephrology. He remained in remission on follow-up.
© The Author(s), 2022.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures

References
-
- Nakazawa D, Masuda S, Tomaru U, et al. Pathogenesis and therapeutic interventions for ANCA-associated vasculitis. Nat Rev Rheumatol 2019; 15: 91–101. - PubMed
-
- Grygiel-Górniak B, Limphaibool N, Perkowska K, et al. Clinical manifestations of granulomatosis with polyangiitis: key considerations and major features. Postgrad Med 2018; 130: 581–596. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous