

Novel technique to fenestrate an aortic dissection flap using electrocautery
- PMID: 37181477
- PMCID: PMC10172989
- DOI: 10.1016/j.jvscit.2023.101108
Novel technique to fenestrate an aortic dissection flap using electrocautery
Abstract
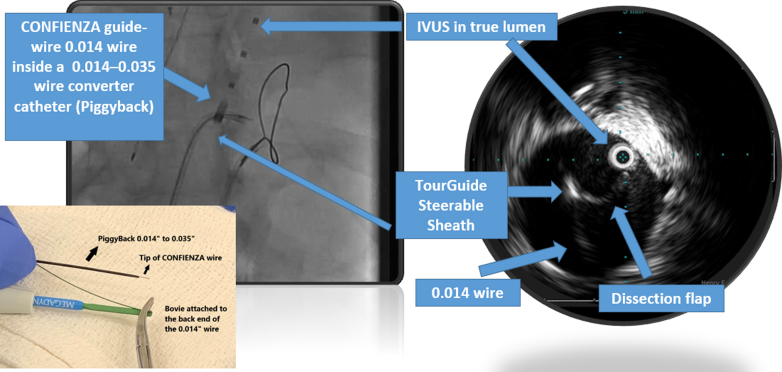
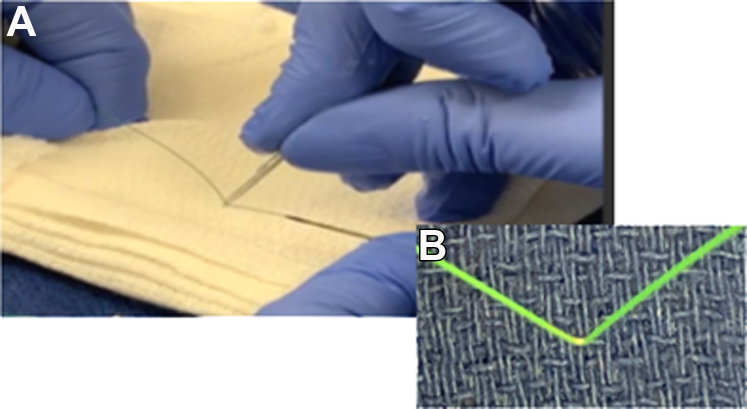
Chronic distal thoracic dissections treated with thoracic endovascular repair are prone to type Ib false lumen perfusion. When the supraceliac aorta is of normal caliber, fenestration of the dissection flap proximal to the visceral vessels creates a seal zone for the thoracic stent graft and eliminates the type Ib false lumen perfusion. We describe a novel way of crossing the septum using electrocautery delivered through a wire tip then fenestrating the septum using electrocautery delivered over a 1-mm area of uninsulated wire to cut the septum. We believe the use of electrocautery creates a controlled and deliberate aortic fenestration during endovascular repair of a distal thoracic dissections.
Keywords: Aortic dissection; Fenestration; Septostomy; TEVAR; Type B aortic dissection.
© 2023 The Author(s).
Figures



References
-
- Tefera G., Acher C.W., Hoch J.R., Mell M., Turnipseed W.D. Effectiveness of intensive medical therapy in type B aortic dissection: a single-center experience. J Vasc Surg. 2007;45:1114–1118. discussion: 8-9. - PubMed
-
- Nienaber C.A., Kische S., Rousseau H., Eggebrecht H., Rehders T.C., Kundt G., et al. Endovascular repair of type B aortic dissection: long-term results of the randomized investigation of stent grafts in aortic dissection trial. Circ Cardiovasc Interv. 2013;6:407–416. - PubMed
-
- Halstead J.C., Meier M., Etz C., Spielvogel D., Bodian C., Wurm M., et al. The fate of the distal aorta after repair of acute type A aortic dissection. J Thorac Cardiovasc Surg. 2007;133:127–135. - PubMed
-
- Subramanian S., Roselli E.E. Thoracic aortic dissection: long-term results of endovascular and open repair. Semin Vasc Surg. 2009;22:61–68. - PubMed
-
- Kabbani L.S., Criado E., Upchurch G.R., Jr., Patel H.J., Eliason J.L., Rectenwald J., et al. Hybrid repair of aortic aneurysms involving the visceral and renal vessels. Ann Vasc Surg. 2010;24:219–224. - PubMed
LinkOut - more resources
Full Text Sources
