

Resection Techniques During Robotic Partial Nephrectomy: A Systematic Review
- PMID: 37182118
- PMCID: PMC10172691
- DOI: 10.1016/j.euros.2023.03.008
Resection Techniques During Robotic Partial Nephrectomy: A Systematic Review
Abstract
Context: The resection technique used to excise tumor during robotic partial nephrectomy (RPN) is of paramount importance in achieving optimal clinical outcomes.
Objective: To provide an overview of the different resection techniques used during RPN, and a pooled analysis of comparative studies.
Evidence acquisition: The systematic review was conducted according to established principles (PROSPERO: CRD42022371640) on November 7, 2022. A population (P: adult patients undergoing RPN), intervention (I: enucleation), comparator (C: enucleoresection or wedge resection), outcome (O: outcome measurements of interest), and study design (S) framework was prespecified to assess study eligibility. Studies reporting a detailed description of resection techniques and/or evaluating the impact of resection technique on outcomes of surgery were included.
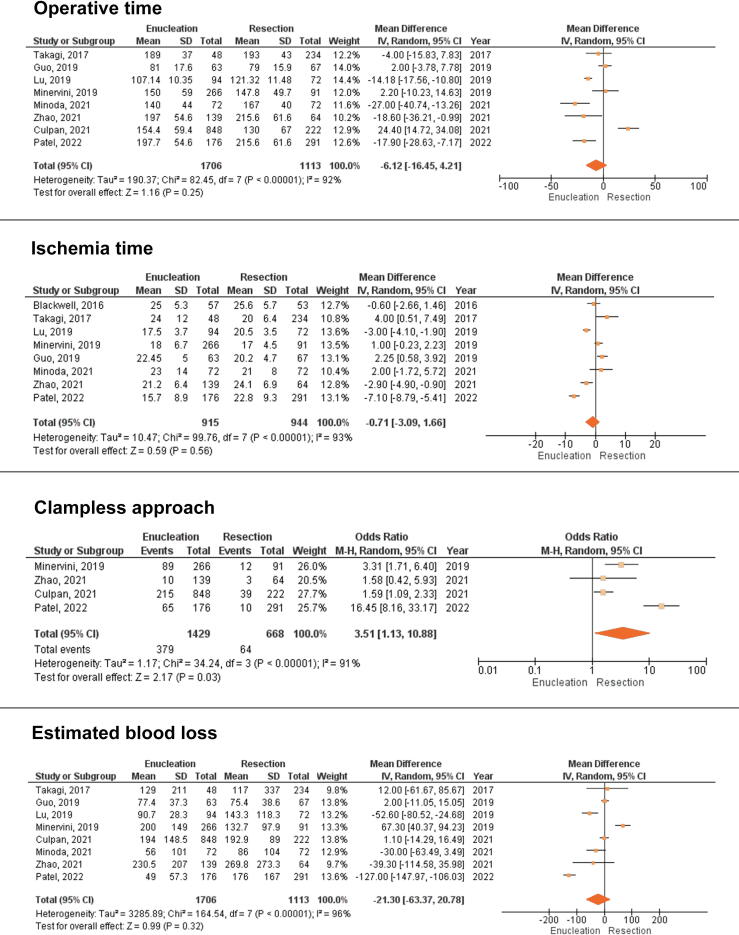
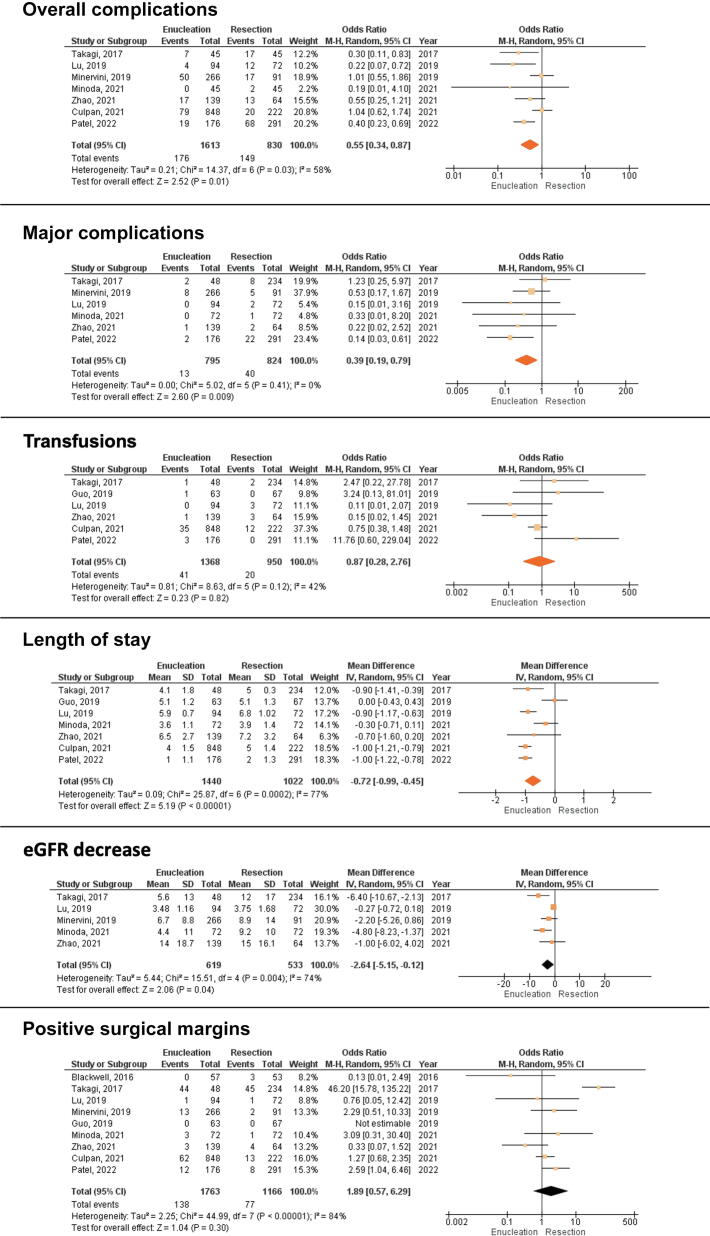
Evidence synthesis: Resection techniques used during RPN can be broadly classified as resection (non-anatomic) or enucleation (anatomic). A standardized definition for these is lacking. Out of 20 studies retrieved, nine compared "standard" resection versus enucleation. A pooled analysis did not reveal significant differences in terms of operative time, ischemia time, blood loss, transfusions, or positive margins. Significant differences favoring enucleation were found for clamping management (odds ratio [OR] for renal artery clamping 3.51, 95% confidence interval [CI] 1.13-10.88; p = 0.03), overall complications (OR for occurrence 0.55, 95% CI 0.34-0.87; p = 0.01) major complications (OR for occurrence 0.39, 95% CI 0.19-0.79; p = 0.009), length of stay (weighted mean difference [WMD] -0.72 d, 95% CI -0.99 to -0.45; p < 0.001), and decrease in estimated glomerular filtration rate (WMD -2.64 ml/min, 95% CI -5.15 to -0.12; p = 0.04).
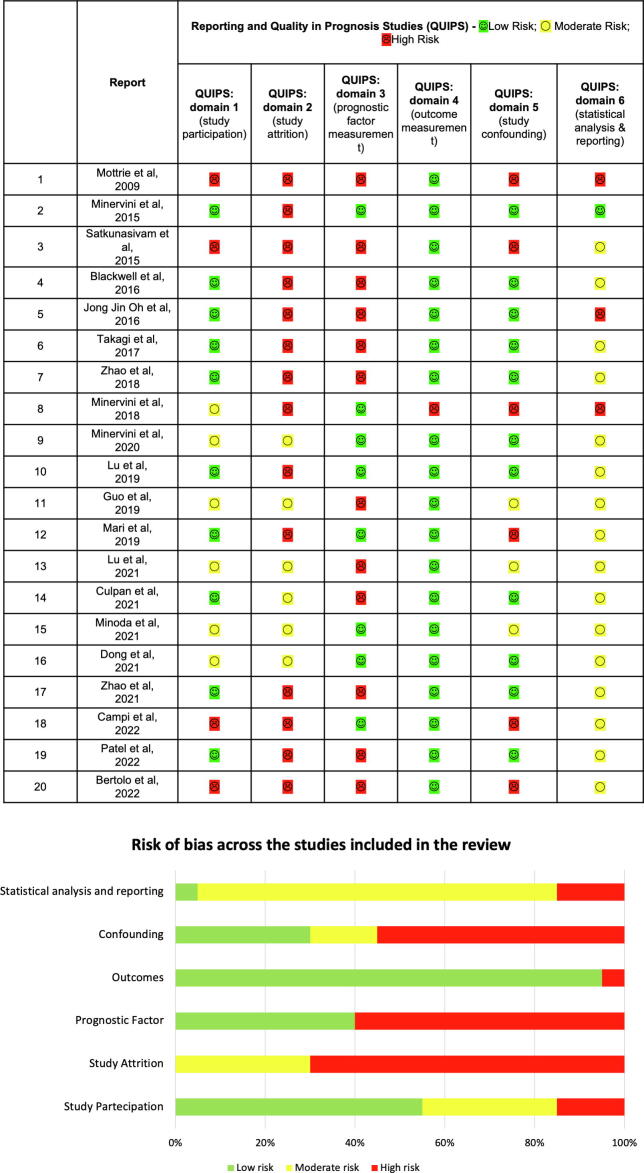
Conclusions: There is heterogeneity in the reporting of resection techniques used during RPN. The urological community must improve the quality of reporting and research produced accordingly. Positive margins are not specifically related to the resection technique. Focusing on studies comparing standard resection versus enucleation, advantages with tumor enucleation in terms of avoidance of artery clamping, overall/major complications, length of stay, and renal function were found. These data should be considered when planning the RPN resection strategy.
Patient summary: We reviewed studies on robotic surgery for partial kidney removal using different techniques to cut away the kidney tumor. We found that a technique called "enucleation" was associated with similar cancer control outcomes in comparison to the standard technique and had fewer complications, better kidney function after surgery, and a shorter hospital stay.
Keywords: Enucleation; Enucleoresection; Outcomes; Partial Nephrectomy; Resection; Robot; Surgery; Technique.
© 2023 The Authors.
Figures

References
-
- Gupta G.N., Boris R.S., Campbell S.C., et al. Tumor enucleation for sporadic localized kidney cancer: pro and con. J Urol. 2015;194:623–625. - PubMed
-
- Minervini A., Campi R., Lane B.R., et al. Impact of resection technique on perioperative outcomes and surgical margins after partial nephrectomy for localized renal masses: a prospective multicenter study. J Urol. 2020;203:496–504. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
