

Cumulative burden of late, major surgical intervention in survivors of childhood cancer: a report from the Childhood Cancer Survivor Study (CCSS) cohort
- PMID: 37182536
- PMCID: PMC10348667
- DOI: 10.1016/S1470-2045(23)00154-7
Cumulative burden of late, major surgical intervention in survivors of childhood cancer: a report from the Childhood Cancer Survivor Study (CCSS) cohort
Abstract
Background: Multimodal cancer therapy places childhood cancer survivors at increased risk for chronic health conditions, subsequent malignancies, and premature mortality as they age. We aimed to estimate the cumulative burden of late (>5 years from cancer diagnosis), major surgical interventions among childhood cancer survivors, compared with their siblings, and to examine associations between specific childhood cancer treatments and the burden of late surgical interventions.
Methods: We analysed data from the Childhood Cancer Survivor Study (CCSS), a retrospective cohort study with longitudinal prospective follow-up of 5-year survivors of childhood cancer (diagnosed before age 21 years) treated at 31 institutions in the USA, with a comparison group of nearest-age siblings of survivors selected by simple random sampling. The primary outcome was any self-reported late, major surgical intervention (defined as any anaesthesia-requiring operation) occurring 5 years or more after the primary cancer diagnosis. The cumulative burden was assessed with mean cumulative counts (MCC) of late, major surgical interventions. Piecewise exponential regression models with calculation of adjusted rate ratios (RRs) evaluated associations between treatment exposures and late, major surgical interventions.
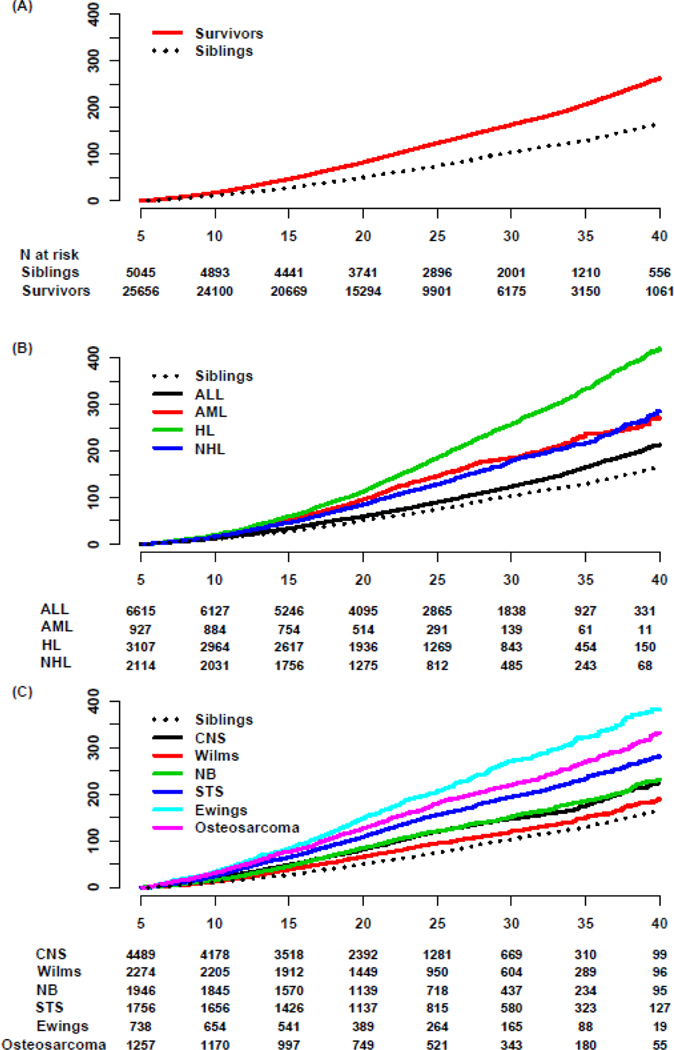
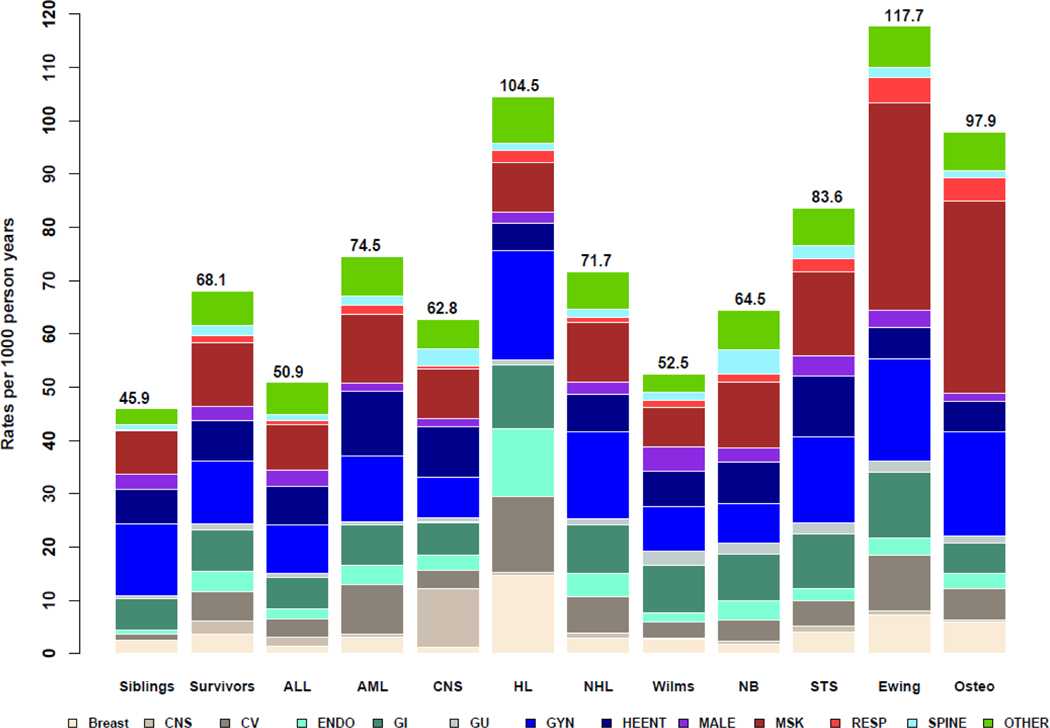
Findings: Between Jan 1, 1970, and Dec 31, 1999, 25 656 survivors were diagnosed (13 721 male, 11 935 female; median follow-up 21·8 years [IQR 16·5-28·4]; median age at diagnosis 6·1 years [3·0-12·4]); 5045 nearest-age siblings were also included as a comparison group. Survivors underwent 28 202 late, major surgical interventions and siblings underwent 4110 late, major surgical interventions. The 35-year MCC of a late, major surgical intervention was 206·7 per 100 survivors (95% CI 202·7-210·8) and 128·9 per 100 siblings (123·0-134·7). The likelihood of a late, major surgical intervention was higher in survivors versus siblings (adjusted RR 1·8, 95% CI 1·7-1·9) and in female versus male survivors (1·4; 1·4-1·5). Survivors diagnosed in the 1990s (adjusted RR 1·4, 95% CI 1·3-1·5) had an increased likelihood of late surgery compared with those diagnosed in the 1970s. Survivors received late interventions more frequently than siblings in most anatomical regions or organ systems, including CNS (adjusted RR 16·9, 95% CI 9·4-30·4), endocrine (6·7, 5·2-8·7), cardiovascular (6·6, 5·2-8·3), respiratory (5·3, 3·4-8·2), spine (2·4, 1·8-3·2), breast (2·1, 1·7-2·6), renal or urinary (2·0, 1·5-2·6), musculoskeletal (1·5, 1·4-1·7), gastrointestinal (1·4, 1·3-1·6), and head and neck (1·2, 1·1-1·4) interventions. Survivors of Hodgkin lymphoma (35-year MCC 333·3 [95% CI 320·1-346·6] per 100 survivors), Ewing sarcoma (322·9 [294·5-351·3] per 100 survivors), and osteosarcoma (269·6 [250·1-289·2] per 100 survivors) had the highest cumulative burdens of late, major surgical interventions. Locoregional surgery or radiotherapy cancer treatment were associated with undergoing late surgical intervention in the same body region or organ system.
Interpretation: Childhood cancer survivors have a significant burden of late, major surgical interventions, a late effect that has previously been poorly quantified. Survivors would benefit from regular health-care evaluations aiming to anticipate impending surgical issues and to intervene early in the disease course when feasible.
Funding: US National Institutes of Health, US National Cancer Institute, American Lebanese Syrian Associated Charities, and St Jude Children's Research Hospital.
Copyright © 2023 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests We declare no competing interests.
Figures
Comment in
-
Long-term surgical consequences of childhood cancer.Lancet Oncol. 2023 Jun;24(6):582-583. doi: 10.1016/S1470-2045(23)00166-3. Epub 2023 May 11. Lancet Oncol. 2023. PMID: 37182537 No abstract available.
-
Late surgical intervention after childhood cancer treatment.Transl Pediatr. 2023 Dec 26;12(12):2093-2094. doi: 10.21037/tp-23-367. Epub 2023 Dec 22. Transl Pediatr. 2023. PMID: 38197109 Free PMC article. No abstract available.
-
Childhood cancer survivors: improving our practice today to reduce late, major surgical interventions tomorrow.Transl Pediatr. 2024 Jan 29;13(1):6-9. doi: 10.21037/tp-23-417. Epub 2024 Jan 5. Transl Pediatr. 2024. PMID: 38323172 Free PMC article. No abstract available.
References
-
- Howlader N, Noone A, Krapcho M, Miller D, Bishop K, Kosary C, et al. SEER Cancer Statistics Review Bethesda, MD: National Cancer Institute; 1975-2014 [Available from: https://seer.cancer.gov/archive/csr/1975_2014/.
-
- Oeffinger KC, Mertens AC, Sklar CA, Kawashima T, Hudson MM, Meadows AT, et al. Chronic health conditions in adult survivors of childhood cancer. N Engl J Med. 2006;355(15):1572–82. - PubMed
-
- Suh E, Stratton KL, Leisenring WM, Nathan PC, Ford JS, Freyer DR, et al. Late mortality and chronic health conditions in long-term survivors of early-adolescent and young adult cancers: a retrospective cohort analysis from the Childhood Cancer Survivor Study. Lancet Oncol. 2020;21(3):421–35. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
