

Pathophysiology and Optimal Treatment of Intracranial Branch Atheromatous Disease
- PMID: 37183021
- PMCID: PMC10322737
- DOI: 10.5551/jat.RV22003
Pathophysiology and Optimal Treatment of Intracranial Branch Atheromatous Disease
Abstract
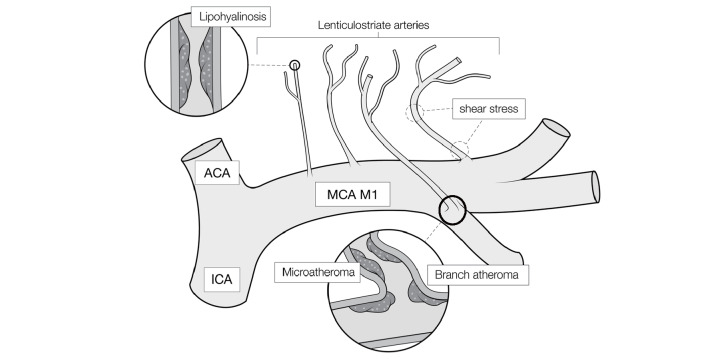
Intracranial branch atheromatous disease (BAD) is a pathological condition characterized by the occlusion of a relatively large perforating branch (700-800 µm) near the orifice of a parent artery due to atherosclerotic plaque-based thrombus (microatheroma). BAD is refractory to treatment and follows a course of progressive exacerbation, especially motor paralysis. Uniform treatment for common atherothrombotic cerebral infarction or lacunar infarction does not prevent the progressive exacerbation of BAD, and consequently affects functional prognosis. To date, various combinations of treatments have been investigated and proposed to attenuate the worsening symptoms of BAD. However, no therapy with established efficacy is yet available for BAD. Since it is the most difficult condition to treat in the area of cerebral infarction, the establishment of optimal treatment methods for BAD is keenly awaited. This review presents an overview of the acute treatments available for BAD and discusses the prospects for optimal treatment.
Keywords: Alteplase; Branch atheromatous disease; Dual-antiplatelet treatment; Lenticulostriate artery.
Conflict of interest statement
The authors declare that no conflicts of interest exist.
Figures
References
-
- Caplan LR: Intracranial branch atheromatous disease: a neglected, understudied, and underused concept. Neurology, 1989; 39: 1246-1250 - PubMed
-
- Fisher CM, and Caplan LR: Basilar artery branch occlusion: a cause of pontine infarction. Neurology, 1971; 21: 900-905 - PubMed
-
- Suto Y, Nakayasu H, Maeda M, Kusumi M, Kowa H, Awaki E, Saito J, and Nakashima K: Long-term prognosis of patients with large subcortical infarctions. Eur Neurol, 2009; 62: 304-310 - PubMed
-
- Aoki J, Iguchi Y, Kimura K, Shibazaki K, Iwanaga T, and Sakai K: Diameter of the basilar artery may be associated with neurological deterioration in acute pontine infarction. Eur Neurol, 2010; 63: 221-226 - PubMed
-
- Kwan MWM, Mak W, Cheung RTF, and Ho SL: Ischemic stroke related to intracranial branch atheromatous disease and comparison with large and small artery diseases. J Neurol Sci, 2011; 303: 80-84 - PubMed