Wound infiltration or transversus abdominis plane block after laparoscopic radical prostatectomy: a randomized clinical trial
- PMID: 37183287
- PMCID: PMC10183622
- DOI: 10.17085/apm.23005
Wound infiltration or transversus abdominis plane block after laparoscopic radical prostatectomy: a randomized clinical trial
Abstract
Background: Regional anesthesia techniques are commonly used for postoperative pain management during laparoscopic surgery. Our aim was to compare the analgesic efficacy of pre-incisional subcutaneous wound infiltration (WI) with that of the transversus abdominis plane (TAP) block as part of a multimodal analgesic approach in laparoscopic radical prostatectomy.
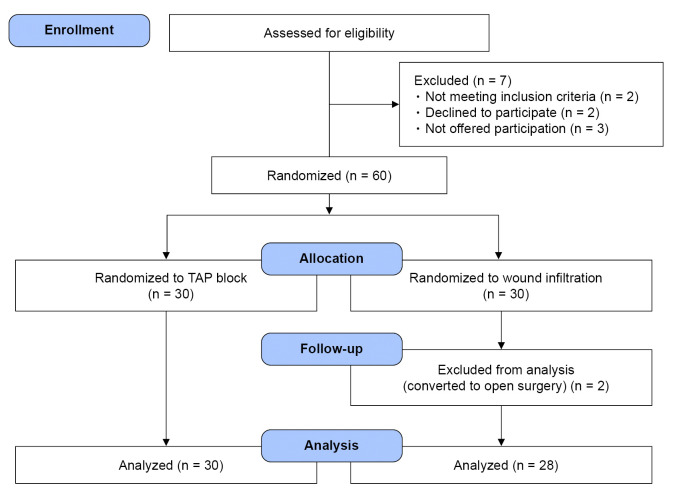
Methods: In this prospective, double-blinded, randomized controlled clinical trial, 60 patients were assigned to either TAP or WI group. The main outcome was acute postoperative pain control assessed using the mean numeric rating scale (NRS) at the 24 hours postoperatively. The secondary outcomes were opioid requirements, procedure-related complications, overall complications, and length of stay.
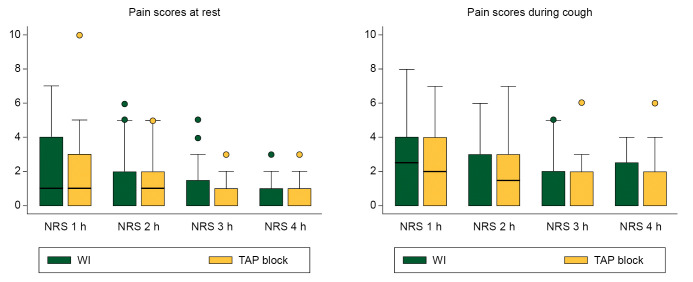
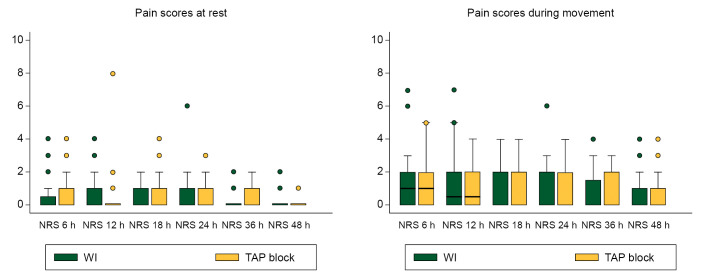
Results: In this study, 60 patients were randomized: 30 to TAP group and 28 to WI (two were excluded due to conversion to open surgery). We found no significant difference in the median (1Q, 3Q) NRS scores during the 24 h postoperatively neither at rest (TAP, 0 (0, 1) vs. WI, 0 (0, 1), P = 0.812), nor during movement (TAP, 1 (0, 2) vs. WI, 1 (0, 2), P = 0.708). There were no statistical differences in the postoperative intravenous morphine requirements in the TAP vs. WI groups during the same period (1.7 ± 3.1 vs. 1.8 ± 4.1 mg; P = 0.910). Only one patient in the TAP group presented with postoperative nausea and vomiting.
Conclusions: Both pre-incisional subcutaneous WI and TAP blockade were associated with very low pain scores as part of a non-opioid multimodal analgesic regimen in laparoscopic radical prostatectomy. This study did not demonstrate the benefits of WI over TAP.
Keywords: Enhanced recovery after surgery; Laparoscopic prostatectomy; Multimodal analgesia; Transversus abdominis plane block; Wound infiltration.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
References
-
- Ilic D, Evans SM, Allan CA, Jung JH, Murphy D, Frydenberg M. Laparoscopic and robot-assisted vs open radical prostatectomy for the treatment of localized prostate cancer: a Cochrane systematic review. BJU Int. 2018;121:845–53. - PubMed
-
- Wagenhoffer R, Gruner M, Schymik J, Schachtner L, Neagoe L, Berg C, et al. Switching from endoscopic extraperitoneal radical prostatectomy to robot-assisted laparoscopic prostatectomy: comparing outcomes and complications. Urol Int. 2015;95:380–5. - PubMed
-
- Bisgaard T, Klarskov B, Rosenberg J, Kehlet H. Characteristics and prediction of early pain after laparoscopic cholecystectomy. Pain. 2001;90:261–9. - PubMed
-
- Joshi GP, Rawal N, Kehlet H, Bonnet F, Camu F, Fischer HB, et al. Evidence-based management of postoperative pain in adults undergoing open inguinal hernia surgery. Br J Surg. 2012;99:168–85. - PubMed
-
- Wick EC, Grant MC, Wu CL. Postoperative multimodal analgesia pain management with nonopioid analgesics and techniques: a review. JAMA Surg. 2017;152:691–7. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous