

Lipoprotein(a) Genotype Influences the Clinical Diagnosis of Familial Hypercholesterolemia
- PMID: 37183858
- PMCID: PMC10227296
- DOI: 10.1161/JAHA.122.029223
Lipoprotein(a) Genotype Influences the Clinical Diagnosis of Familial Hypercholesterolemia
Abstract
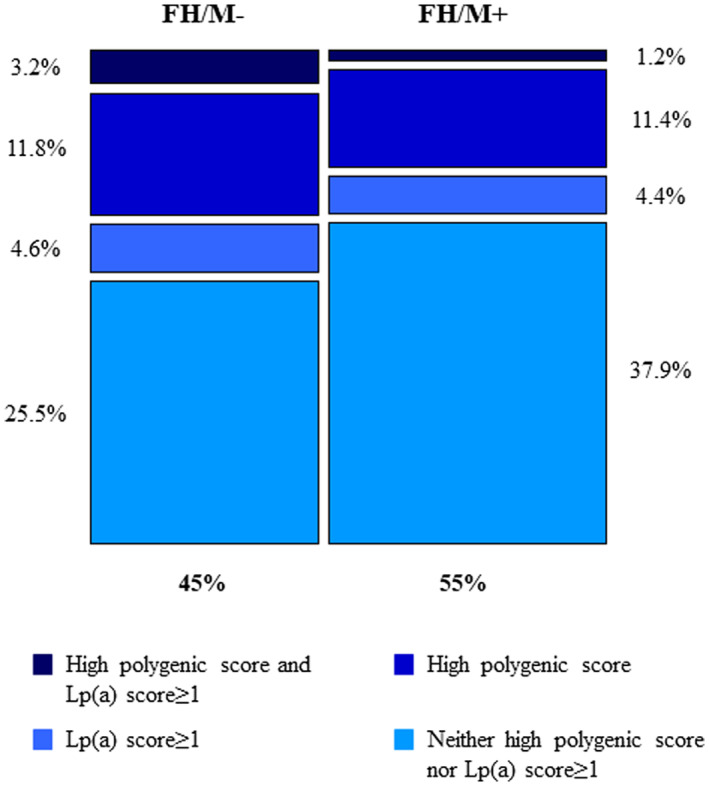
Background Evidence suggests that LPA risk genotypes are a possible contributor to the clinical diagnosis of familial hypercholesterolemia (FH). This study aimed at determining the prevalence of LPA risk variants in adult individuals with FH enrolled in the Italian LIPIGEN (Lipid Transport Disorders Italian Genetic Network) study, with (FH/M+) or without (FH/M-) a causative genetic variant. Methods and Results An lp(a) [lipoprotein(a)] genetic score was calculated by summing the number risk-increasing alleles inherited at rs3798220 and rs10455872 variants. Overall, in the 4.6% of 1695 patients with clinically diagnosed FH, the phenotype was not explained by a monogenic or polygenic cause but by genotype associated with high lp(a) levels. Among 765 subjects with FH/M- and 930 subjects with FH/M+, 133 (17.4%) and 95 (10.2%) were characterized by 1 copy of either rs10455872 or rs3798220 or 2 copies of either rs10455872 or rs3798220 (lp(a) score ≥1). Subjects with FH/M- also had lower mean levels of pretreatment low-density lipoprotein cholesterol than individuals with FH/M+ (t test for difference in means between FH/M- and FH/M+ groups <0.0001); however, subjects with FH/M- and lp(a) score ≥1 had higher mean (SD) pretreatment low-density lipoprotein cholesterol levels (223.47 [50.40] mg/dL) compared with subjects with FH/M- and lp(a) score=0 (219.38 [54.54] mg/dL for), although not statistically significant. The adjustment of low-density lipoprotein cholesterol levels based on lp(a) concentration reduced from 68% to 42% the proportion of subjects with low-density lipoprotein cholesterol level ≥190 mg/dL (or from 68% to 50%, considering a more conservative formula). Conclusions Our study supports the importance of measuring lp(a) to perform the diagnosis of FH appropriately and to exclude that the observed phenotype is driven by elevated levels of lp(a) before performing the genetic test for FH.
Keywords: cardiovascular risk; clinical diagnosis; familial hypercholesterolemia; lipoprotein(a).
Figures
References
-
- Nordestgaard BG, Chapman MJ, Humphries SE, Ginsberg HN, Masana L, Descamps OS, Wiklund O, Hegele RA, Raal FJ, Defesche JC, et al. Familial hypercholesterolaemia is underdiagnosed and undertreated in the general population: guidance for clinicians to prevent coronary heart disease: consensus statement of the European Atherosclerosis Society. Eur Heart J. 2013;34:3478–3490. doi: 10.1093/eurheartj/eht273 - DOI - PMC - PubMed
-
- Olmastroni E, Gazzotti M, Arca M, Averna M, Pirillo A, Catapano AL, Casula M, Groupdagger LS. Twelve variants polygenic score for low‐density lipoprotein cholesterol distribution in a large cohort of patients with clinically diagnosed familial hypercholesterolemia with or without causative mutations. J Am Heart Assoc. 2022;11:e023668. doi: 10.1161/JAHA.121.023668 - DOI - PMC - PubMed
-
- Utermann G, Hoppichler F, Dieplinger H, Seed M, Thompson G, Boerwinkle E. Defects in the low density lipoprotein receptor gene affect lipoprotein (a) levels: multiplicative interaction of two gene loci associated with premature atherosclerosis. Proc Natl Acad Sci USA. 1989;86:4171–4174. doi: 10.1073/pnas.86.11.4171 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
