

Identification of vulnerable carotid plaque with histologically validated CT-derived plaque maps
- PMID: 37183910
- PMCID: PMC10321253
- DOI: 10.1259/bjr.20220982
Identification of vulnerable carotid plaque with histologically validated CT-derived plaque maps
Abstract
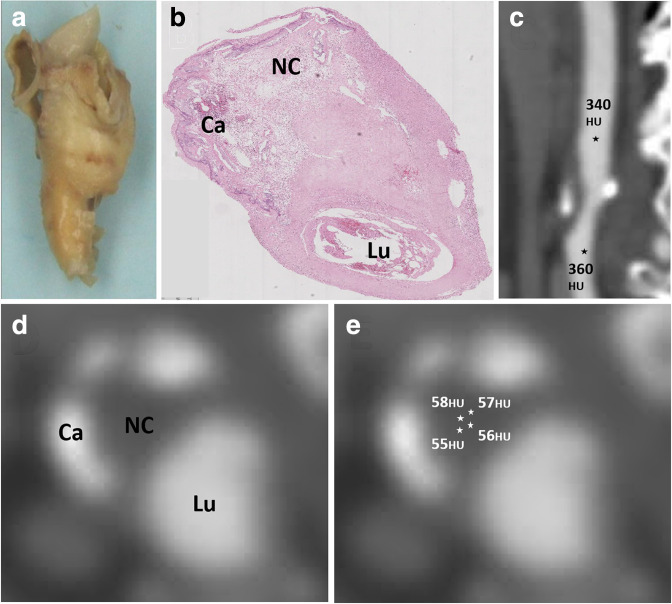
Objectives: Ruptured carotid plaque causes stroke, but differentiating rupture-prone necrotic core from fibrous tissue with CT is limited by overlap of X-ray attenuation. We investigated the ability of CT-derived plaque maps created from ratios of plaque/contrast attenuation to identify histologically proven vulnerable plaques.
Methods: Seventy patients underwent carotid CT angiography and carotid endarterectomy. A derivation cohort of 20 patients had CT images matched with histology and carotid plaque components attenuation defined. In a validation cohort of 50 patients, CT-derived plaque maps were compared in 43 symptomatic vs 40 asymptomatic carotid plaques and accuracy detecting vulnerable plaques calculated.
Results: In 250 plaque areas co-registered with histology, the median attenuation (HU) of necrotic core 43(26-63), fibrous plaque 127(110-162) and calcified plaque 964 (816-1207) created significantly different ratios of plaque/contrast attenuation. CT-derived plaque maps revealed symptomatic plaques had larger necrotic core than asymptomatic (13.5%(5.9-33.3) vs 7.4%(2.3-14.3), p = 0.004) with large necrotic core predicting symptoms (area under ROC curve 0.68, p = 0.004). Twenty-four of 47 carotid plaques were histologically classified as most vulnerable (Starry-Type VI). Plaque maps revealed Type VI plaques had a greater necrotic core volume than Type IV/V plaques and a necrotic core/fibrous plaque ratio >0.5 distinguished Type VI plaques with sensitivity 75.0% (55.1-88.0) and specificity of 39.1% (22.2-59.2).
Conclusions: Carotid plaque components can be differentiated by CT using a ratio of plaque/contrast attenuation. CT-derived plaque map volumes of necrotic core help distinguished the most vulnerable plaques.
Advances in knowledge: CT-derived plaque maps based on plaque/contrast attenuation may provide new markers of carotid plaque vulnerability.
Figures




References
-
- Kernan WN, Ovbiagele B, Black HR, Bravata DM, Chimowitz MI, Ezekowitz MD, et al. . Guidelines for the prevention of stroke in patients with stroke and transient ischemic attack: A guideline for healthcare professionals from the American heart association/American stroke association. Stroke 2014; 45: 2160–2236. doi: 10.1161/STR.0000000000000024 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
