

Population-Based Estimates for the Prevalence of Multiple Sclerosis in the United States by Race, Ethnicity, Age, Sex, and Geographic Region
- PMID: 37184850
- PMCID: PMC10186207
- DOI: 10.1001/jamaneurol.2023.1135
Population-Based Estimates for the Prevalence of Multiple Sclerosis in the United States by Race, Ethnicity, Age, Sex, and Geographic Region
Abstract
Importance: Racial, ethnic, and geographic differences in multiple sclerosis (MS) are important factors to assess when determining the disease burden and allocating health care resources.
Objective: To calculate the US prevalence of MS in Hispanic, non-Hispanic Black (hereafter referred to as Black), and non-Hispanic White individuals (hereafter referred to as White) stratified by age, sex, and region.
Design, setting, and participants: A validated algorithm was applied to private, military, and public (Medicaid and Medicare) administrative health claims data sets to identify adult cases of MS between 2008 and 2010. Data analysis took place between 2019 and 2022. The 3-year cumulative prevalence overall was determined in each data set and stratified by age, sex, race, ethnicity, and geography. The insurance pools included 96 million persons from 2008 to 2010. Insurance and stratum-specific estimates were applied to the 2010 US Census data and the findings combined to calculate the 2010 prevalence of MS cumulated over 10 years. No exclusions were made if a person met the algorithm criteria.
Main outcomes and measurements: Prevalence of MS per 100 000 US adults stratified by demographic group and geography. The 95% CIs were approximated using a binomial distribution.
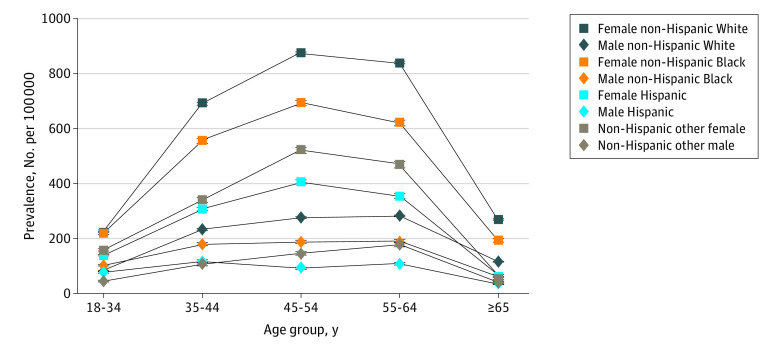
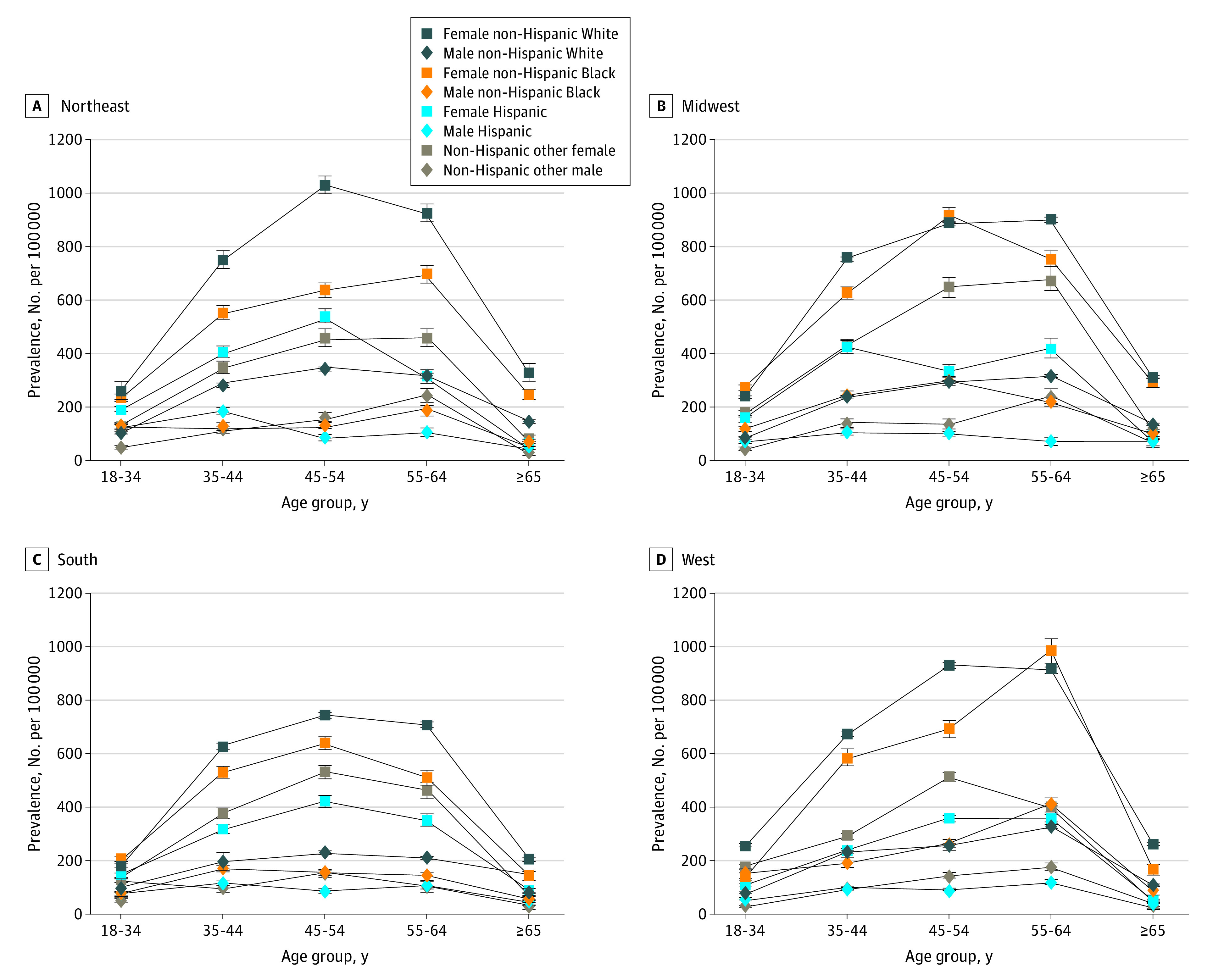
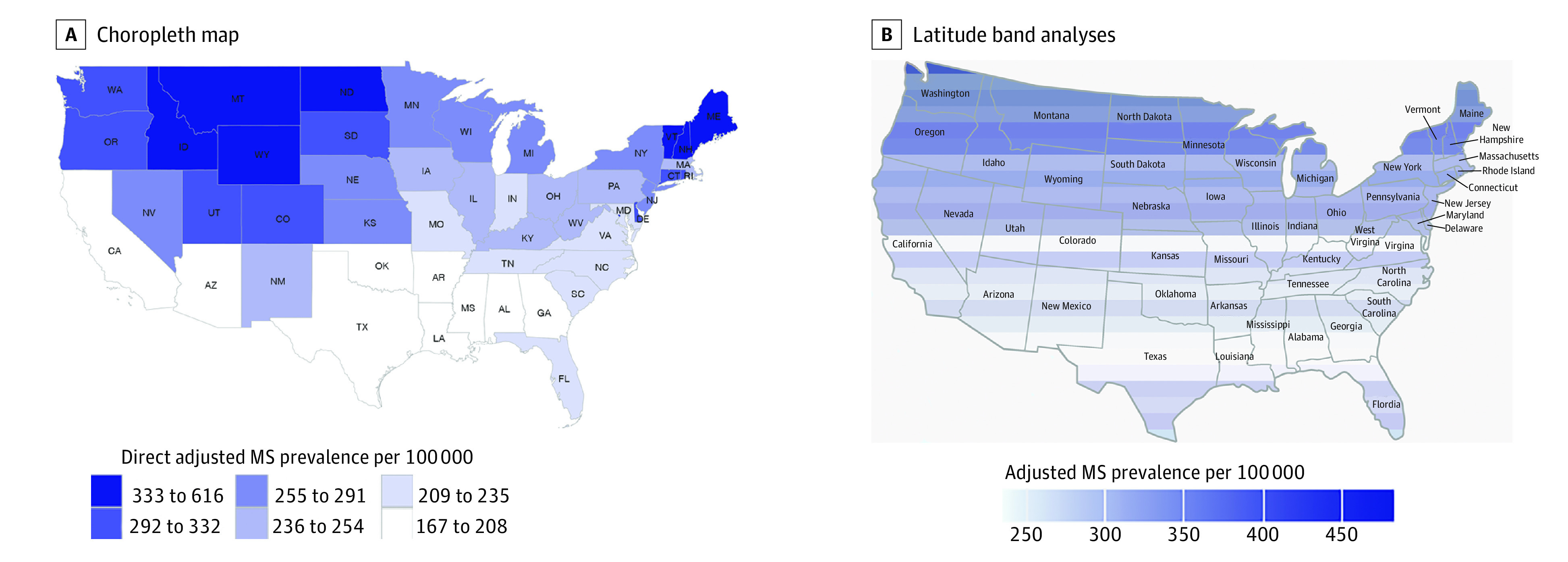
Results: A total of 744 781 persons 18 years and older were identified with MS with 564 426 cases (76%) in females and 180 355 (24%) in males. The median age group was 45 to 54 years, which included 229 216 individuals (31%), with 101 271 aged 18 to 24 years (14%), 158 997 aged 35 to 44 years (21%), 186 758 aged 55 to 64 years (25%), and 68 539 individuals (9%) who were 65 years or older. White individuals were the largest group, comprising 577 725 cases (77%), with 80 276 Black individuals (10%), 53 456 Hispanic individuals (7%), and 33 324 individuals (4%) in the non-Hispanic other category. The estimated 2010 prevalence of MS per 100 000 US adults cumulated over 10 years was 161.2 (95% CI, 159.8-162.5) for Hispanic individuals (regardless of race), 298.4 (95% CI, 296.4-300.5) for Black individuals, 374.8 (95% CI, 373.8-375.8) for White individuals, and 197.7 (95% CI, 195.6-199.9) for individuals from non-Hispanic other racial and ethnic groups. During the same time period, the female to male ratio was 2.9 overall. Age stratification in each of the racial and ethnic groups revealed the highest prevalence of MS in the 45- to 64-year-old age group, regardless of racial and ethnic classification. With each degree of latitude, MS prevalence increased by 16.3 cases per 100 000 (95% CI, 12.7-19.8; P < .001) in the unadjusted prevalence estimates, and 11.7 cases per 100 000 (95% CI, 7.4-16.1; P < .001) in the direct adjusted estimates. The association of latitude with prevalence was strongest in women, Black individuals, and older individuals.
Conclusions and relevance: This study found that White individuals had the highest MS prevalence followed by Black individuals, individuals from other non-Hispanic racial and ethnic groups, and Hispanic individuals. Inconsistent racial and ethnic classifications created heterogeneity within groups. In the United States, MS affects diverse racial and ethnic groups. Prevalence of MS increases significantly and nonuniformly with latitude in the United States, even when adjusted for race, ethnicity, age, and sex. These findings are important for clinicians, researchers, and policy makers.
Conflict of interest statement
Figures
Comment in
-
Making Sure Multiple Sclerosis Counts and Is Counted for All-An Update on Multiple Sclerosis Prevalence by Race and Ethnicity in the United States.JAMA Neurol. 2023 Jul 1;80(7):667-669. doi: 10.1001/jamaneurol.2023.0469. JAMA Neurol. 2023. PMID: 37184874 No abstract available.
References
-
- Frey WA. Diversity Explosion: How New Racial Demographics Are Remaking America. Brookings Institution Press; 2018:1-20.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
