

Combining Neurocognitive and Functional Tests to Improve Return-to-Sport Decisions Following ACL Reconstruction
- PMID: 37186672
- PMCID: PMC10847844
- DOI: 10.2519/jospt.2023.11489
Combining Neurocognitive and Functional Tests to Improve Return-to-Sport Decisions Following ACL Reconstruction
Abstract
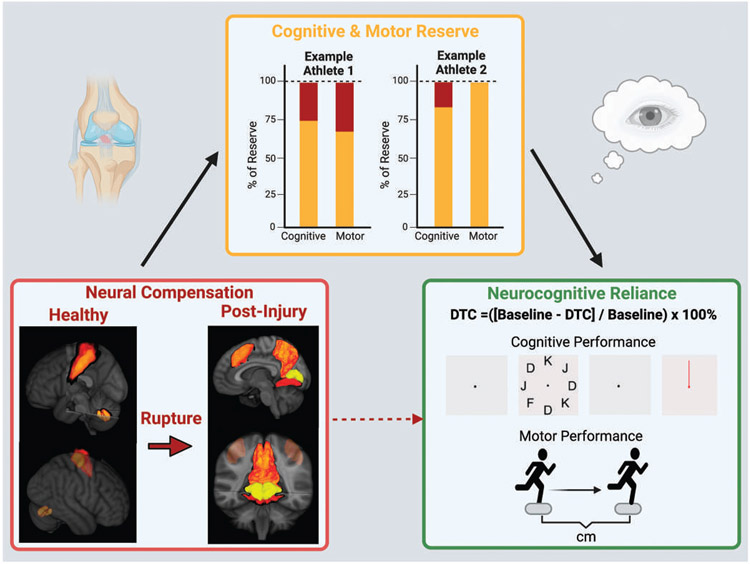
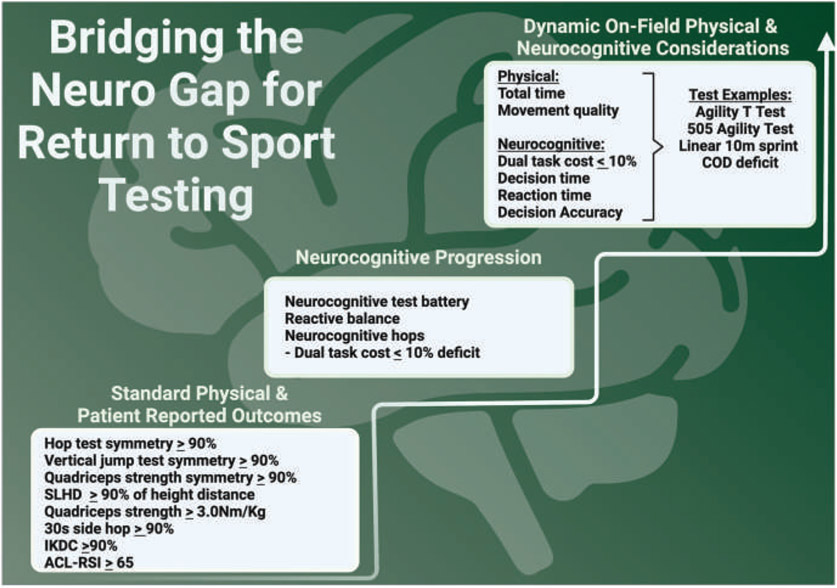
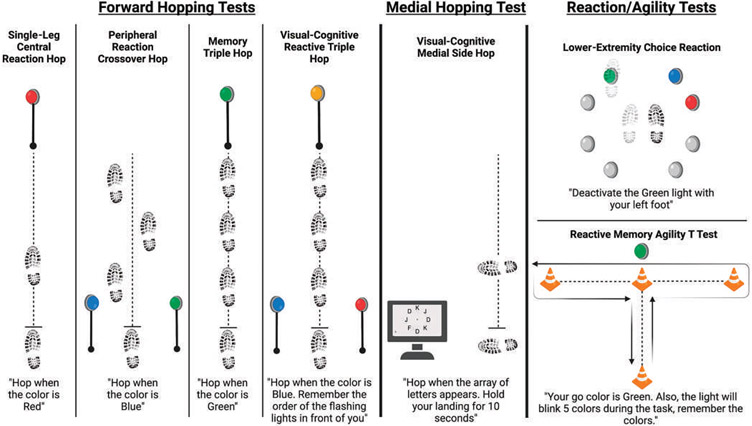
SYNOPSIS: Neuroplasticity after anterior cruciate ligament (ACL) injury alters how the nervous system generates movement and maintains dynamic joint stability. The postinjury neuroplasticity can cause neural compensations that increase reliance on neurocognition. Return-to-sport testing quantifies physical function but fails to detect important neural compensations. To assess for neural compensations in a clinical setting, we recommend evaluating athletes' neurocognitive reliance by augmenting return-to-sport testing with combined neurocognitive and motor dual-task challenges. In this Viewpoint, we (1) share the latest evidence related to ACL injury neuroplasticity and (2) share simple principles and new assessments with preliminary data to improve return-to-sport decisions following ACL reconstruction. J Orthop Sports Phys Ther 2023;53(8):1-5. Epub: 16 May 2023. doi:10.2519/jospt.2023.11489.
Keywords: ACL; fMRI; functional magnetic resonance imaging; knee; motor control/learning; neural control; neuroimaging; neuroscience.
Figures
References
-
- Chaput M, Farraye B, Simon J, Kim H, Monfort S, Grooms D. American Academy of Sports Physical Therapy Platform Presentation Abstracts (SPL1-SPL75). J Orthop Sports Phys Ther. 2022;52:CSM25–CSM54. 10.2519/jospt.2022.52.1.CSM25 - DOI
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical