

Outcomes of Surgical Treatment of Migraines: A Systematic Review & Meta-Analysis
- PMID: 37188139
- PMCID: PMC10170648
- DOI: 10.1177/22925503211036701
Outcomes of Surgical Treatment of Migraines: A Systematic Review & Meta-Analysis
Abstract
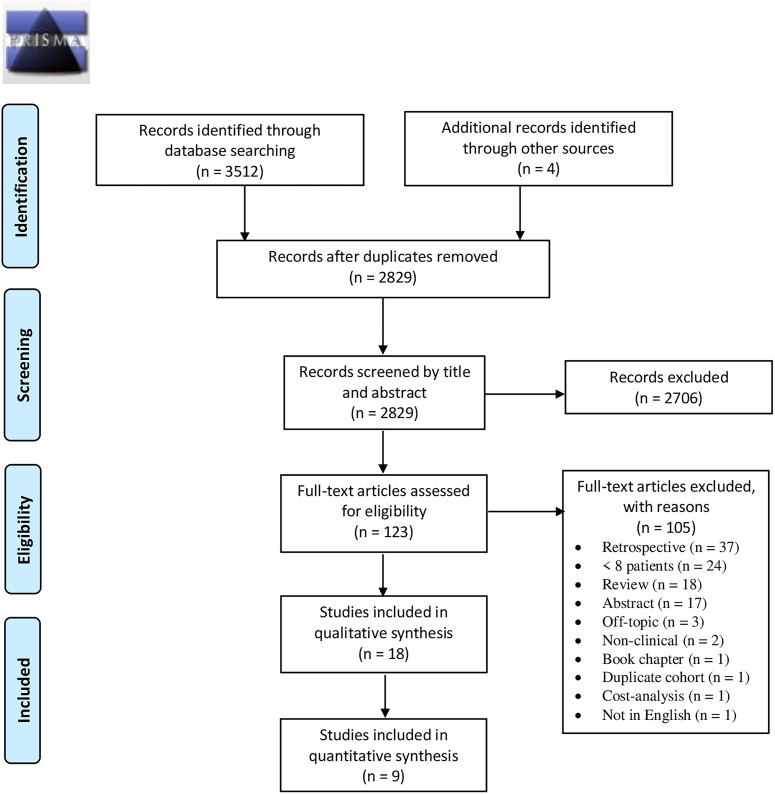
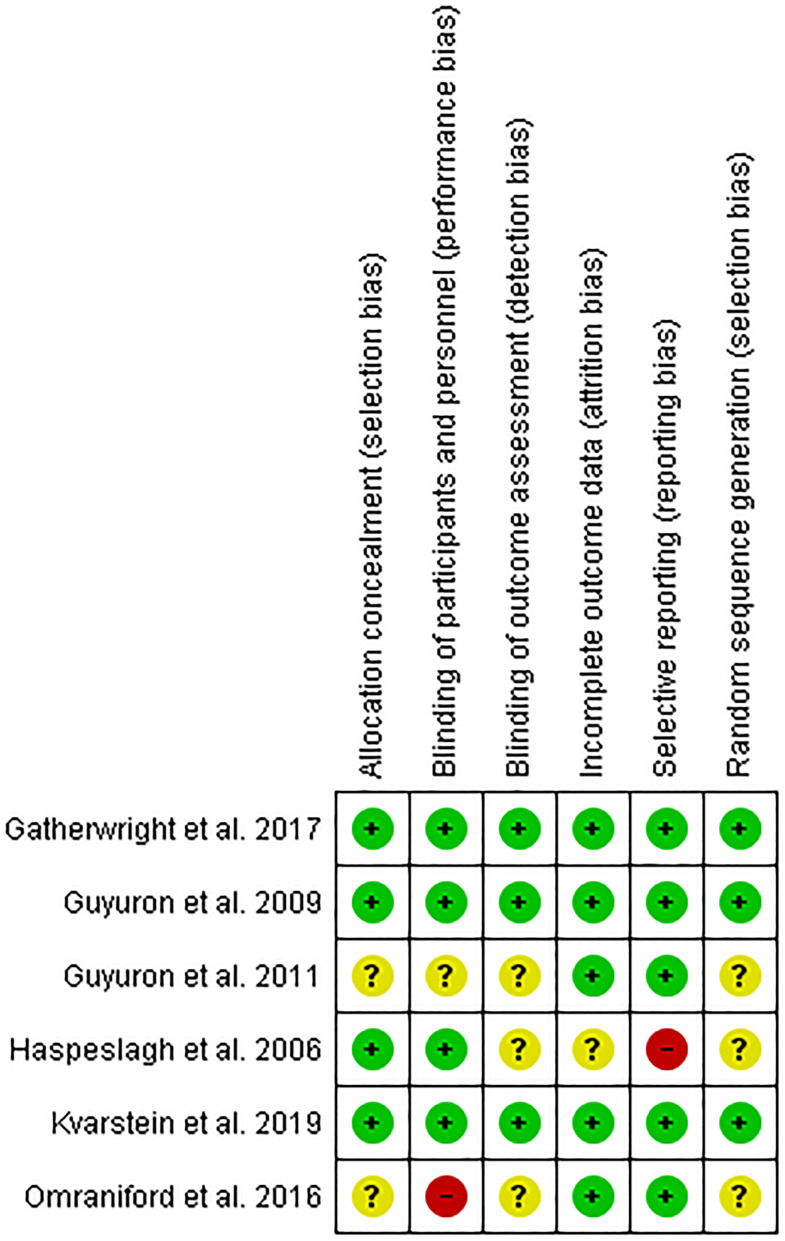
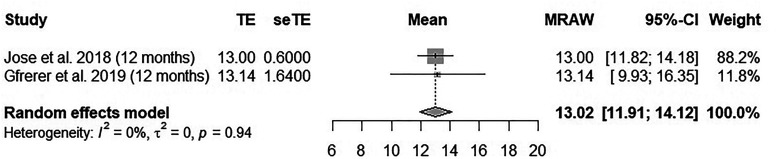
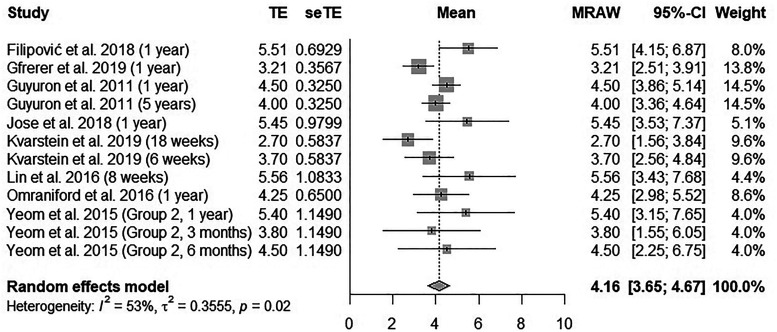
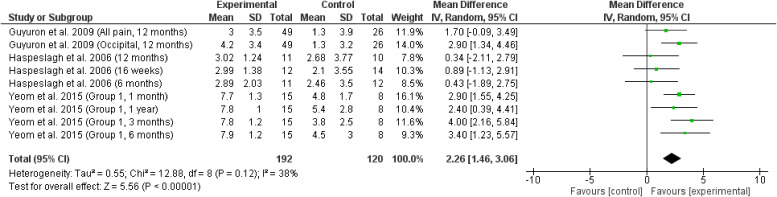
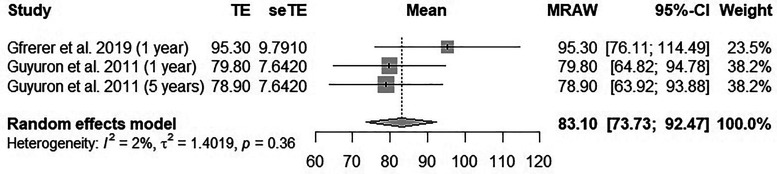
Background: Migraine surgery at 1 of 6 identified "trigger sites" of a target cranial sensory nerve has rapidly grown in popularity since 2000. This study summarizes the effect of migraine surgery on headache severity, headache frequency, and the migraine headache index score which is derived by multiplying migraine severity, frequency, and duration. Materials and Methods: This is a PRISMA-compliant systematic review of 5 databases searched from inception through May 2020 and is registered under the PROSPERO ID: CRD42020197085. Clinical trials treating headaches with surgery were included. Risk of bias was assessed in randomized controlled trials. Meta-analyses were performed on outcomes using a random effects model to determine the pooled mean change from baseline and when possible, to compare treatment to control. Results: 18 studies met criteria including 6 randomized controlled trials, 1 controlled clinical trial, and 11 uncontrolled clinical trials treated 1143 patients with pathologies including migraine, occipital migraine, frontal migraine, occipital nerve triggered headache, frontal headache, occipital neuralgia, and cervicogenic headache. Migraine surgery reduced headache frequency at 1 year postoperative by 13.0 days per month as compared to baseline (I2 = 0%), reduced headache severity at 8 weeks to 5 years postoperative by 4.16 points on a 0 to 10 scale as compared to baseline (I2 = 53%), and reduced migraine headache index at 1 to 5 years postoperative by 83.1 points as compared to baseline (I2 = 2%). These meta-analyses are limited by a small number of studies that could be analyzed, including studies with high risk of bias. Conclusion: Migraine surgery provided a clinically and statistically significant reduction in headache frequency, severity, and migraine headache index scores. Additional studies, including randomized controlled trials with low risk-of-bias should be performed to improve the precision of the outcome improvements.
Historique: Le traitement de la migraine à l’une des six « zones gâchettes » établies d’un nerf crânien sensoriel cible ont rapidement gagné en popularité depuis 2000. La présente étude résume l’effet du traitement chirurgical de la migraine sur la gravité et la fréquence des céphalées et sur le score de migraine obtenu par la multiplication de la gravité, de la fréquence et de la durée des migraines. Matériel et méthodologie: La présente analyse systématique de cinq bases de données fouillées depuis leur création jusqu’à mai 2020 respecte la liste PRISMA et est enregistrée sous le numéro d’identification CRD42020197085 de PROSPERO. Les chercheurs ont retenu les études cliniques sur le traitement des céphalées par des interventions chirurgicales. Ils ont évalué le risque de biais des études aléatoires et contrôlées. Ils ont également effectué des méta-analyses des résultats au moyen d’un modèle à effets aléatoires pour déterminer le changement moyen regroupé par rapport à l’état de référence et, dans la mesure du possible, pour comparer des sujets traités à des sujets témoins. Résultats: Au total, 18 études respectaient les critères, y compris six études aléatoires et contrôlées, une étude clinique contrôlée, et 11 études non contrôlées auprès de 1 143 patients ayant des pathologies incluant la migraine, la migraine occipitale, la migraine frontale, la céphalée occipitale, la céphalée frontale, la névralgie occipitale et la céphalée cervicogénique. Par rapport à l’état de départ, le traitement chirurgical de la migraine avait réduit la fréquence des céphalées de 13,0 jours par mois (I2 = 0%) un an après l’opération, la gravité des céphalées de 4,16 points sur une échelle de 0 à 10 de huit semaines à cinq ans après l’opération (I2 = 53%) et le score de migraine de 83,1 points de un à cinq ans après l’opération (I2 = 2%). Ces méta-analyses sont limitées par le petit nombre d’études pouvant être analysées, y compris des études comportant de forts risques de biais. Conclusion: Le traitement chirurgical de la migraine assure une diminution cliniquement et statistiquement significative de la fréquence et de la gravité des céphalées, ainsi que des scores de migraine. D’autres études, y compris des études aléatoires et contrôlées comportant un faible risque de biais, devront être exécutées pour mieux préciser les améliorations aux résultats cliniques.
Keywords: headache; migraine disorders; migraine surgery; neuralgia; reconstructive surgical procedures; treatment outcome.
© 2021 The Author(s).
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
-
- Migraine is an extraordinarily prevalent neurological disease, affecting 39 million men, women and children in the U.S. and 1 billion worldwide. Migraine Research Foundation. https://migraineresearchfoundation.org/about-migraine/migraine-facts/. Accessed 11/26/2020.
LinkOut - more resources
Full Text Sources
Miscellaneous