

Management of Atypical Central Serous Chorioretinopathy Mimicking Vogt-Koyanagi-Harada Disease
- PMID: 37188205
- PMCID: PMC10170611
- DOI: 10.1177/24741264231152675
Management of Atypical Central Serous Chorioretinopathy Mimicking Vogt-Koyanagi-Harada Disease
Abstract
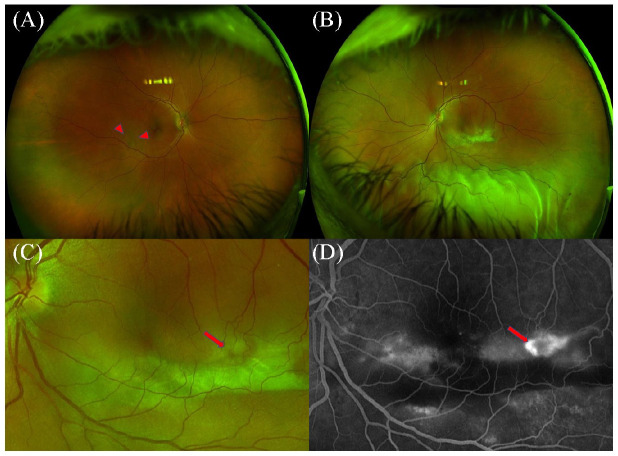
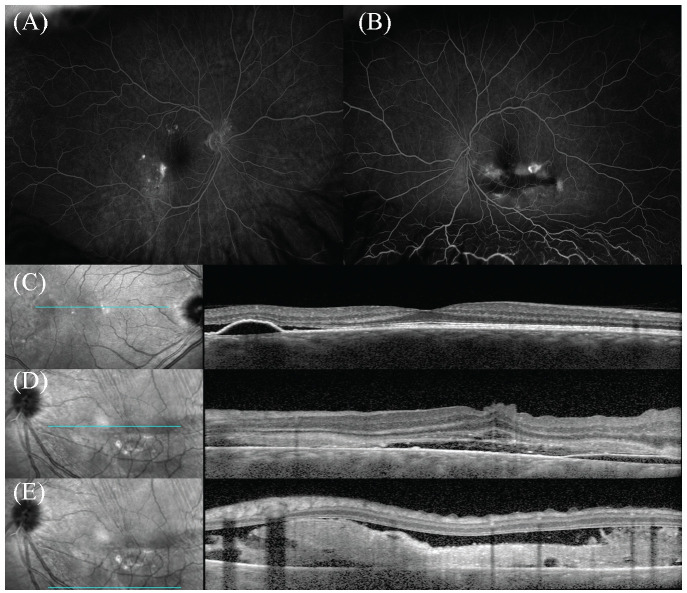
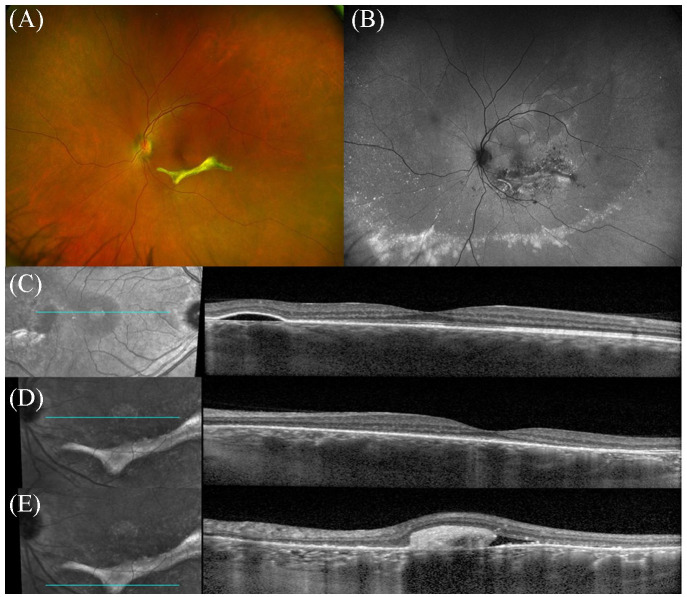
Purpose: To report a case of multifocal central serous chorioretinopathy (CSCR) mimicking Vogt-Koyanagi-Harada (VKH) disease. Methods: A 42-year-old man was evaluated for an exudative retinal detachment (RD) with a presumptive diagnosis of VKH while being treated with corticosteroids. The examination showed subretinal fibrin deposition with a bullous, exudative, macula-involved RD in the left eye and a progressive decline in visual acuity (VA) to hand motions. Multimodal imaging showed multifocal hyperfluorescent leaks bilaterally by angiography, highly suggestive of CSCR exacerbated by corticosteroids. Results: After the multifocal CSCR diagnosis, the systemic corticosteroids were tapered and eventually discontinued. The patient was then managed with focal laser photocoagulation, photodynamic therapy, and acetazolamide. The VA improved to 20/30 with complete resolution of the bullous RD at the 12-month follow-up. Conclusions: Extensive bullous RD with subretinal fibrin deposition is an infrequent manifestation of CSCR commonly associated with corticosteroid use that can mimic VKH. Thus, it is important to distinguish CSCR from VKH and the potential of combination therapy in managing chronic multifocal CSCR with a bullous RD.
Keywords: Vogt-Koyanagi-Harada; central serous chorioretinopathy; corticosteroids; retinal detachment.
© The Author(s) 2023.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
-
- Aggarwal K, Agarwal A, Deokar A, et al.. Distinguishing features of acute Vogt-Koyanagi-Harada disease and acute central serous chorioretinopathy on optical coherence tomography angiography and en face optical coherence tomography imaging. J Ophthalmic Inflamm Infect. 2017;7(1):3. doi:10.1186/s12348-016-0122-z - DOI - PMC - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
