

Left main bifurcation stenting: impact of residual ischaemia on cardiovascular mortality
- PMID: 37188864
- PMCID: PMC10627280
- DOI: 10.1093/eurheartj/ehad318
Left main bifurcation stenting: impact of residual ischaemia on cardiovascular mortality
Abstract
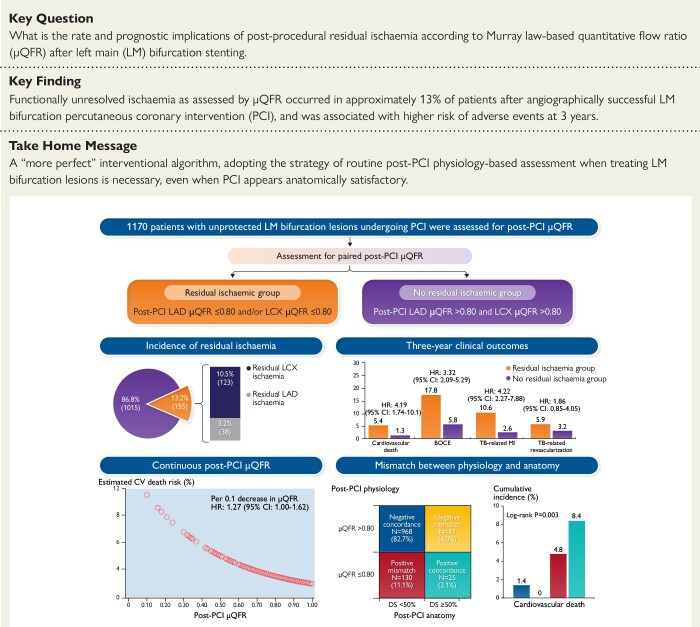
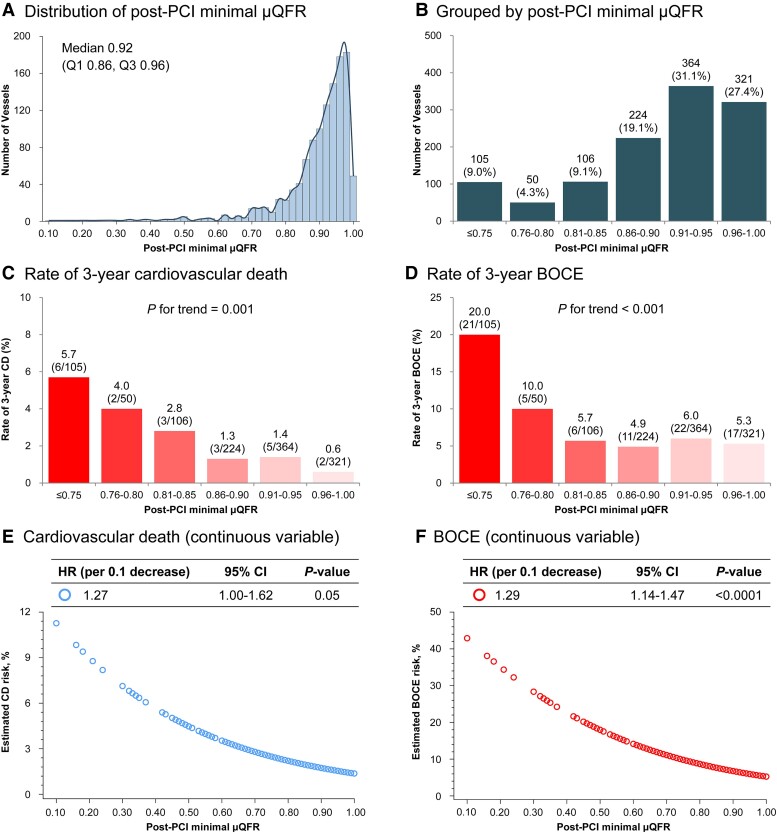
Aims: The present study sought to determine the rate and prognostic implications of post-procedural physiologically significant residual ischemia according to Murray law-based quantitative flow ratio (μQFR) after left main (LM) bifurcation percutaneous coronary intervention (PCI).
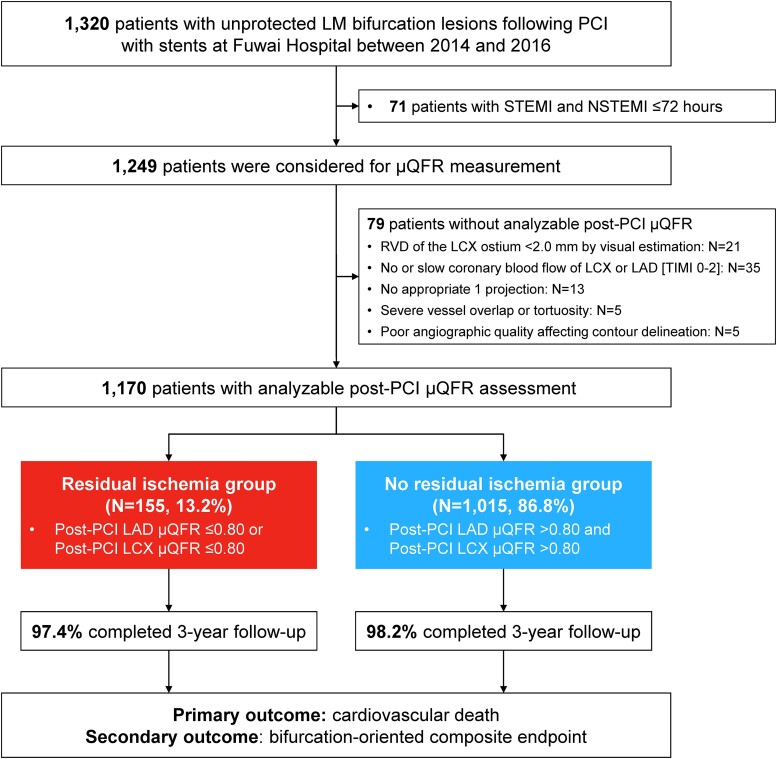
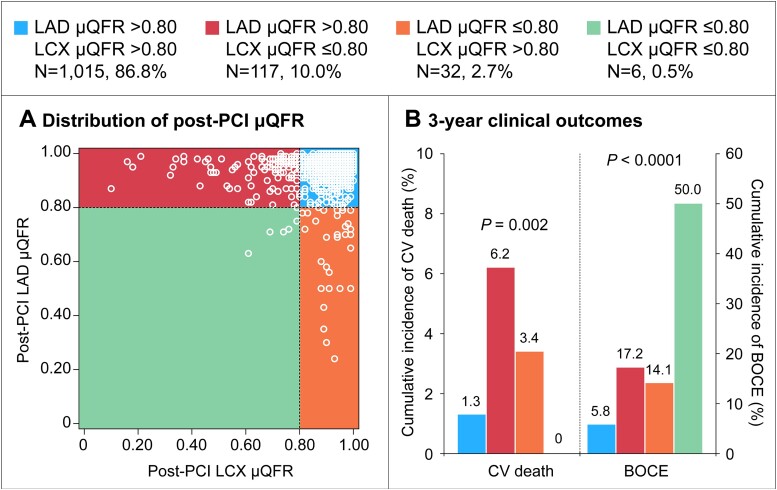
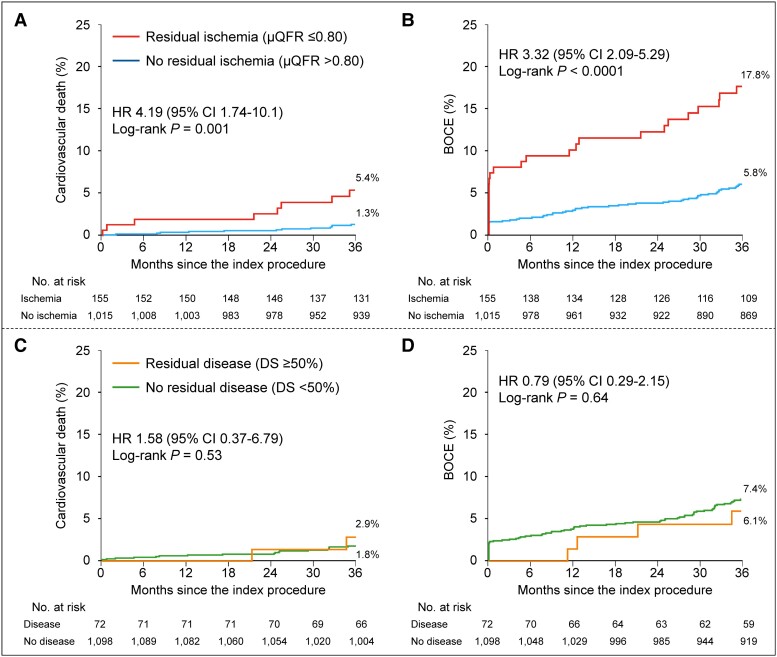
Methods and results: Consecutive patients undergoing LM bifurcation stenting at a large tertiary care center between January 2014 and December 2016 with available post-PCI μQFR were included. Physiologically significant residual ischemia was defined by post-PCI μQFR values ≤0.80 in the left anterior descending (LAD) or left circumflex artery (LCX). The primary outcome was 3-year cardiovascular death. The major secondary outcome was 3-year bifurcation-oriented composite endpoint (BOCE). Among 1170 included patients with analyzable post-PCI μQFR, 155 (13.2%) had residual ischemia in either LAD or LCX. Patients with vs. those without residual ischemia had a higher risk of 3-year cardiovascular mortality [5.4% vs. 1.3%; adjusted hazard ratio (HR) 3.20, 95% confidence interval (CI): 1.16-8.80]. The 3-year risk of BOCE was significantly higher in the residual ischemia group (17.8% vs. 5.8%; adjusted HR 2.79, 95% CI: 1.68-4.64), driven by higher incidence of the composite of cardiovascular death and target bifurcation-related myocardial infarction (14.0% vs. 3.3%; adjusted HR 4.06, 95% CI: 2.22-7.42). A significant, inverse association was observed between continuous post-PCI μQFR and the risk of clinical outcomes (per 0.1 μQFR decrease, HR of cardiovascular death 1.27, 95% CI: 1.00-1.62; HR of BOCE 1.29, 95% CI: 1.14-1.47).
Conclusion: After angiographically successful LM bifurcation PCI, residual ischemia assessed by μQFR was identified in 13.2% of patients and was associated with higher risk of 3-year cardiovascular death, indicating the superior prognostic value of post-PCI physiological assessment.
Keywords: Cardiovascular death; Left main coronary artery disease; Percutaneous coronary intervention; Quantitative flow ratio; Residual ischemia.
© The Author(s) 2023. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of Interest Dr W.W. reports grants and consulting fees from MicroPort, outside the submitted work; is a medical advisor for Rede Optimus and Corrib Core Laboratory; and is a co-founder of Argonauts, an innovation facilitator. Dr S.T. reports research support from Pulse medical imaging technology. All other authors declare no conflict of interest for this contribution.
Figures
Comment in
-
Left main PCI: beware the circumflex!Eur Heart J. 2023 Nov 1;44(41):4337-4339. doi: 10.1093/eurheartj/ehad434. Eur Heart J. 2023. PMID: 37477204 No abstract available.
References
-
- Lawton JS, Tamis-Holland JE, Bangalore S, Bates ER, Beckie TM, Bischoff JM, et al. 2021 ACC/AHA/SCAI guideline for coronary artery revascularization: executive summary: a report of the American College of Cardiology/American Heart Association joint committee on clinical practice guidelines. J Am Coll Cardiol 2022;79:197–215. 10.1016/j.jacc.2021.09.005 - DOI - PubMed
-
- Sabatine MS, Bergmark BA, Murphy SA, O'Gara PT, Smith PK, Serruys PW, et al. Percutaneous coronary intervention with drug-eluting stents versus coronary artery bypass grafting in left main coronary artery disease: an individual patient data meta-analysis. Lancet 2021;398:2247–2257. 10.1016/s0140-6736(21)02334-5 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
