

Tongue necrosis secondary to giant cell arteritis, successfully treated with tocilizumab: a case report
- PMID: 37189114
- PMCID: PMC10184098
- DOI: 10.1186/s12891-023-06465-z
Tongue necrosis secondary to giant cell arteritis, successfully treated with tocilizumab: a case report
Abstract
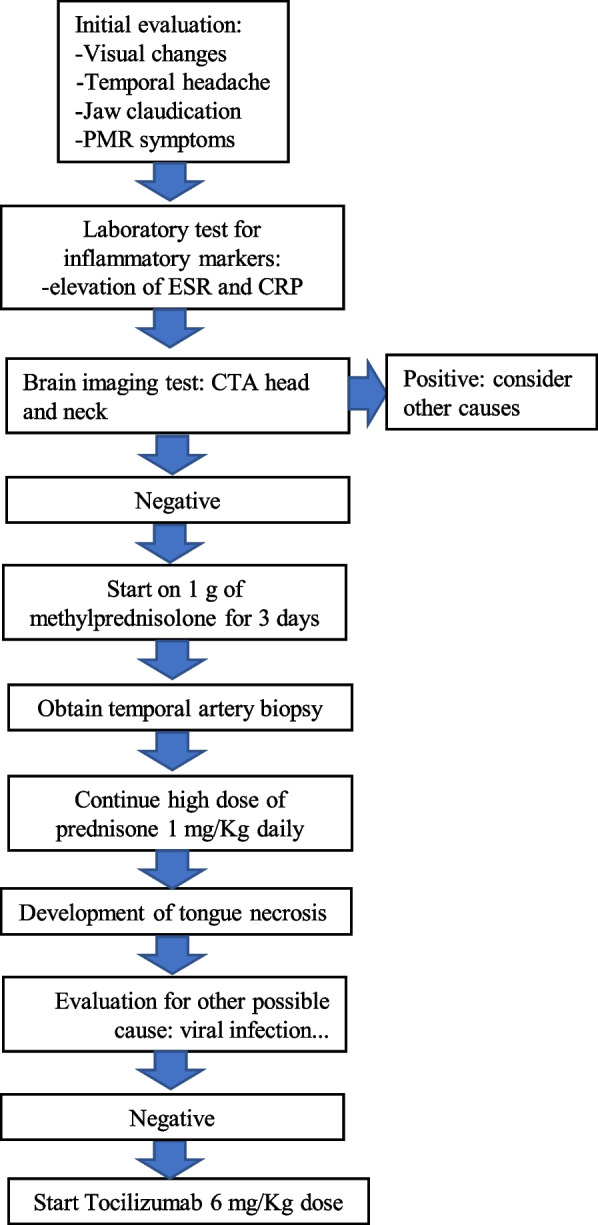
Background: Giant Cell Arteritis (GCA) is a large vessel vasculitis that most commonly presents with headache, scalp tenderness, jaw claudication, and vision changes. Various other, less common, manifestations have been reported in the literature such as scalp and tongue necrosis. Though most patients respond to corticosteroids, some cases of GCA are refractory to the high doses of corticosteroids.
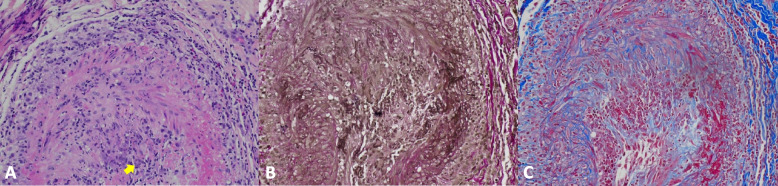
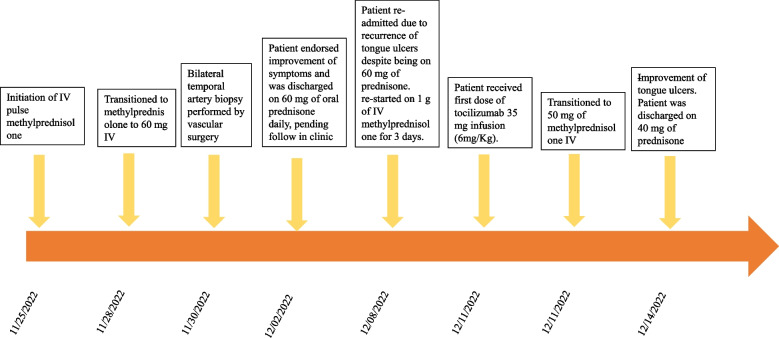
Case presentation: We present a 73-year-old female with GCA refractory to corticosteroids presenting with tongue necrosis. This patient significantly improved with a dose of tocilizumab, an IL-6 inhibitor.
Conclusion: To the best of our knowledge, this is the first case report of a patient with refractory GCA presenting with tongue necrosis that had rapid improvement with tocilizumab. Prompt diagnosis and treatment can prevent severe outcomes such as tongue amputation in GCA patients with tongue necrosis, and tocilizumab may be effective for corticosteroid-refractory cases.
Keywords: Case report; Giant cell arteritis; Refractory; Tocilizumab; Tongue necrosis.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

Similar articles
-
Giant cell arteritis associated with scalp, tongue or lip necrosis: A French multicenter case control study.Semin Arthritis Rheum. 2024 Feb;64:152348. doi: 10.1016/j.semarthrit.2023.152348. Epub 2023 Dec 10. Semin Arthritis Rheum. 2024. PMID: 38091870
-
Tocilizumab in giant cell arteritis: Multicenter open-label study of 22 patients.Semin Arthritis Rheum. 2015 Jun;44(6):717-23. doi: 10.1016/j.semarthrit.2014.12.005. Epub 2014 Dec 27. Semin Arthritis Rheum. 2015. PMID: 25697557
-
Subtotal tongue necrosis in delayed diagnosed giant-cell arteritis: a case report.Am J Otolaryngol. 2004 Nov-Dec;25(6):438-41. doi: 10.1016/j.amjoto.2004.06.004. Am J Otolaryngol. 2004. PMID: 15547815
-
Scalp necrosis in giant cell arteritis: case report and review of the relevance of this cutaneous sign of large-vessel vasculitis.J Am Acad Dermatol. 2009 Oct;61(4):701-6. doi: 10.1016/j.jaad.2008.11.913. Epub 2009 Jul 3. J Am Acad Dermatol. 2009. PMID: 19577329 Review.
-
Tocilizumab for the treatment of giant cell arteritis.Expert Rev Clin Immunol. 2018 May;14(5):339-349. doi: 10.1080/1744666X.2018.1468251. Epub 2018 May 9. Expert Rev Clin Immunol. 2018. PMID: 29676602 Review.
Cited by
-
[Necrosis of the tongue as a clinical manifestation of giant cell arteritis].Inn Med (Heidelb). 2024 May;65(5):508-511. doi: 10.1007/s00108-023-01607-w. Epub 2023 Oct 20. Inn Med (Heidelb). 2024. PMID: 37861722 Free PMC article. German.
-
Calcification following tongue necrosis induced by vasopressor use in a nonintubated patient with septic shock: a case report.J Med Case Rep. 2024 Sep 19;18(1):458. doi: 10.1186/s13256-024-04796-6. J Med Case Rep. 2024. PMID: 39294651 Free PMC article.
-
Lingual Necrosis in the Setting of Giant Cell Arteritis.Cureus. 2024 Nov 23;16(11):e74316. doi: 10.7759/cureus.74316. eCollection 2024 Nov. Cureus. 2024. PMID: 39717321 Free PMC article.
References
-
- Dotiwala AK, Samra NS. Anatomy, head and neck, tongue. 2018. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
