

Somatic Copy Number Alteration in Circulating Tumor DNA for Monitoring of Pediatric Patients with Cancer
- PMID: 37189699
- PMCID: PMC10135914
- DOI: 10.3390/biomedicines11041082
Somatic Copy Number Alteration in Circulating Tumor DNA for Monitoring of Pediatric Patients with Cancer
Erratum in
-
Correction: Ruas et al. Somatic Copy Number Alteration in Circulating Tumor DNA for Monitoring of Pediatric Patients with Cancer. Biomedicines 2023, 11, 1082.Biomedicines. 2025 Nov 25;13(12):2872. doi: 10.3390/biomedicines13122872. Biomedicines. 2025. PMID: 41463134 Free PMC article.
Abstract
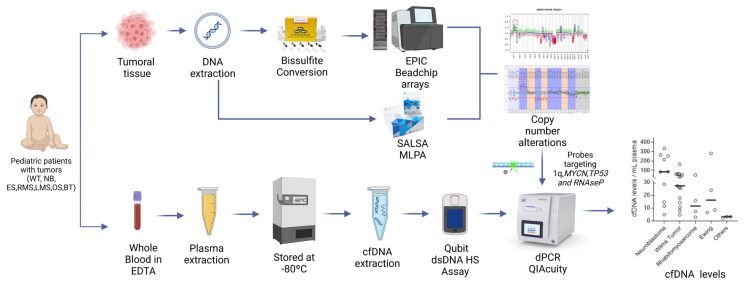
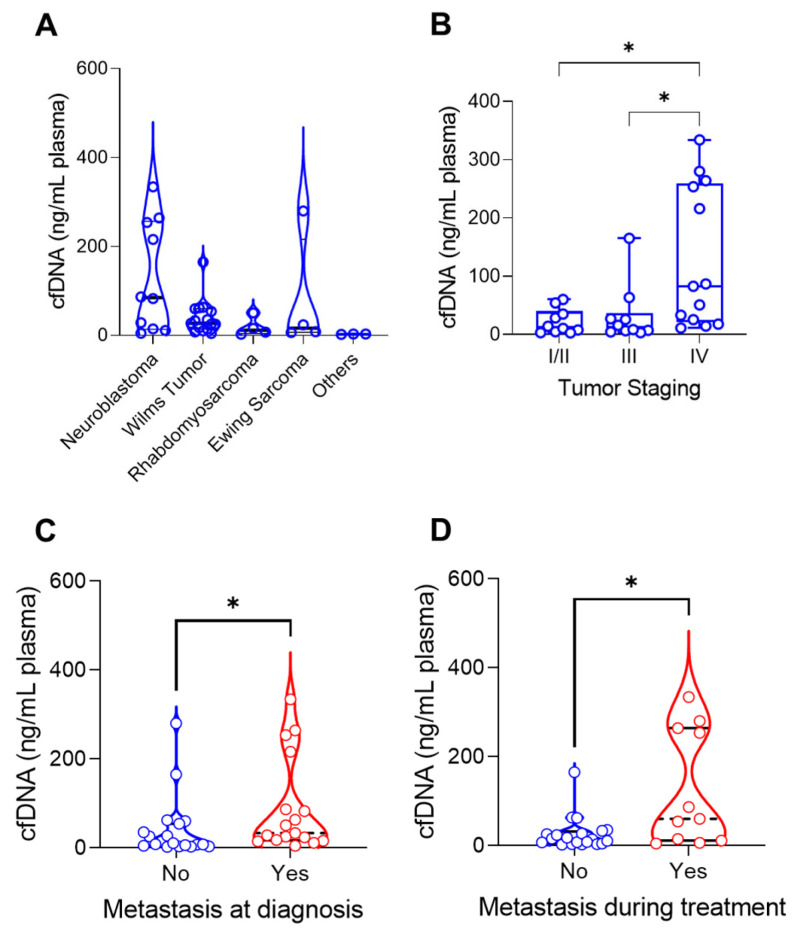
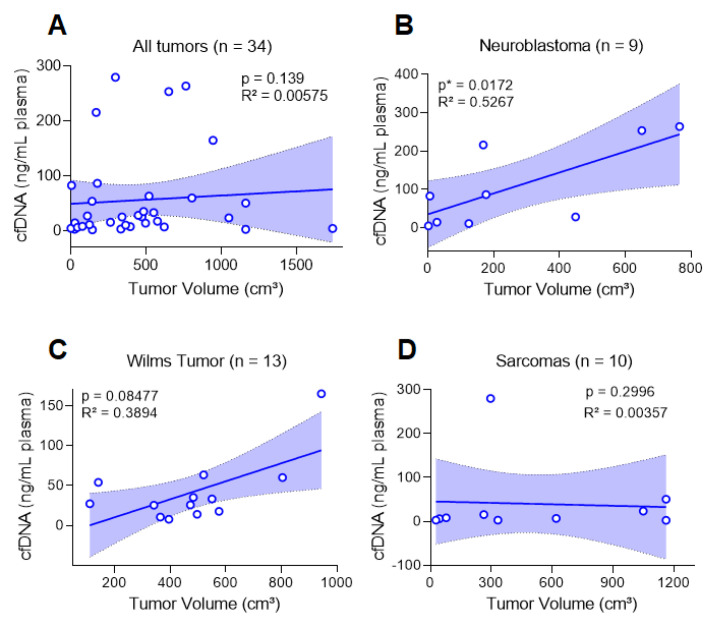
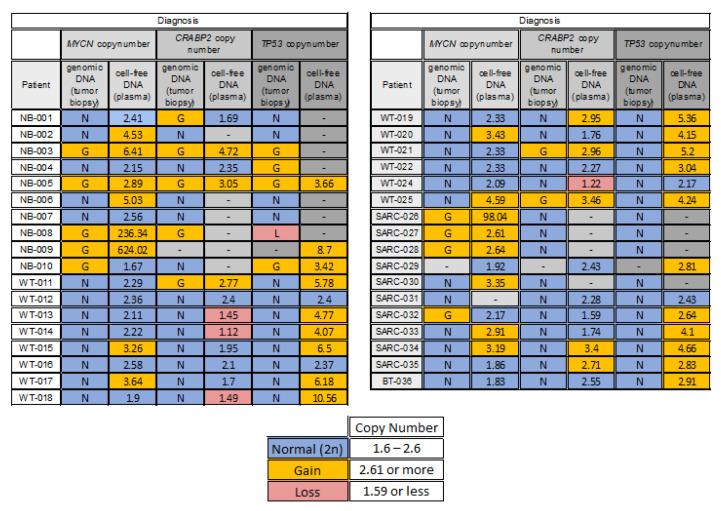
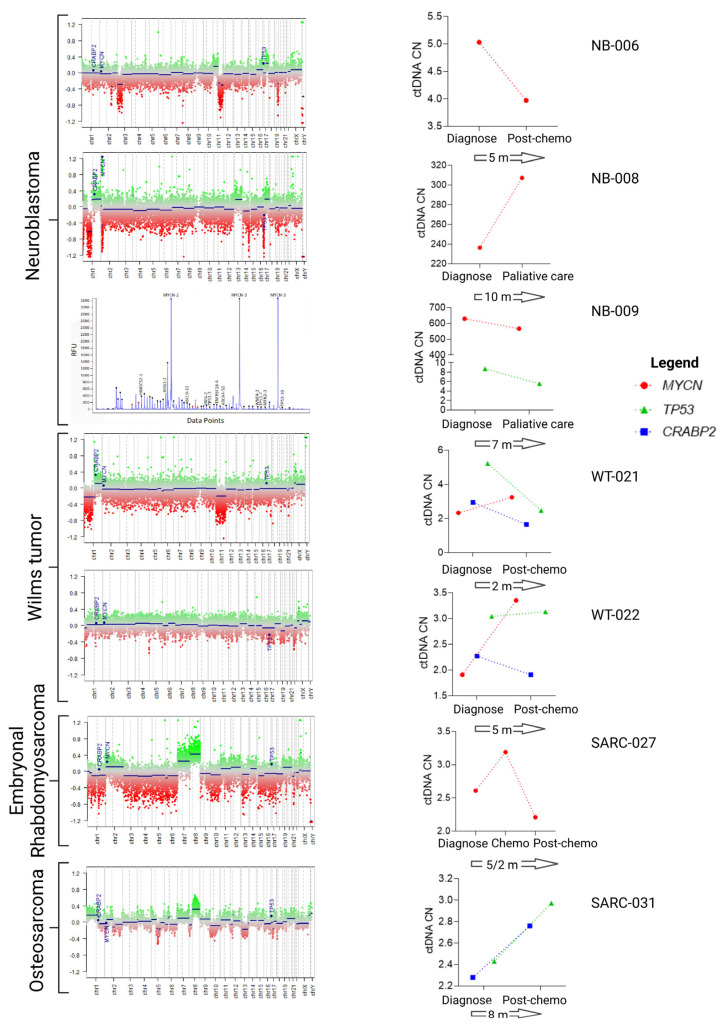
Pediatric tumors share few recurrent mutations and are instead characterized by copy number alterations (CNAs). The cell-free DNA (cfDNA) is a prominent source for the detection of cancer-specific biomarkers in plasma. We profiled CNAs in the tumor tissues for further evaluation of alterations in 1q, MYCN and 17p in the circulating tumor DNA (ctDNA) in the peripheral blood at diagnosis and follow-up using digital PCR. We report that among the different kinds of tumors (neuroblastoma, Wilms tumor, Ewing sarcoma, rhabdomyosarcoma, leiomyosarcoma, osteosarcoma and benign teratoma), neuroblastoma presented the greatest amount of cfDNA, in correlation with tumor volume. Considering all tumors, cfDNA levels correlated with tumor stage, metastasis at diagnosis and metastasis developed during therapy. In the tumor tissue, at least one CNA (at CRABP2, TP53, surrogate markers for 1q and 17p, respectively, and MYCN) was observed in 89% of patients. At diagnosis, CNAs levels were concordant between tumor and ctDNA in 56% of the cases, and for the remaining 44%, 91.4% of the CNAs were present only in cfDNA and 8.6% only in the tumor. Within the cfDNA, we observed that 46% and 23% of the patients had MYCN and 1q gain, respectively. The use of specific CNAs as targets for liquid biopsy in pediatric patients with cancer can improve diagnosis and should be considered for monitoring of the disease response.
Keywords: 1q; MYCN; cell-free DNA; circulating tumor DNA; copy number alterations; digital PCR.
Conflict of interest statement
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Figures
References
-
- Dehner L.P. The Evolution of the Diagnosis and Understanding of Primitive and Embryonic Neoplasms in Children: Living through an Epoch. [(accessed on 1 March 2023)];Mod. Pathol. 1998 11:669–685. Available online: https://pubmed.ncbi.nlm.nih.gov/9688189/ - PubMed
-
- Steliarova-Foucher E., Stiller C., Lacour B., Kaatsch P. International Classification of Childhood Cancer, third edition. [(accessed on 1 March 2023)];Cancer. 2005 103:1457–1467. doi: 10.1002/cncr.20910. Available online: https://pubmed.ncbi.nlm.nih.gov/15712273/ - DOI - PubMed
-
- Tulla M., Berthold F., Graf N., Rutkowski S., von Schweinitz D., Spix C., Kaatsch P. Incidence, Trends, and Survival of Children with Embryonal Tumors. [(accessed on 1 March 2023)];Pediatrics. 2015 136:e623–e632. doi: 10.1542/peds.2015-0224. Available online: https://pubmed.ncbi.nlm.nih.gov/26304823/ - DOI - PubMed
-
- Gröbner S.N., Worst B.C., Weischenfeldt J., Buchhalter I., Kleinheinz K., Rudneva V.A., Johann P.D., Balasubramanian G.P., Segura-Wang M., Brabetz S., et al. The landscape of genomic alterations across childhood cancers. [(accessed on 25 January 2023)];Nature. 2018 555:321–327. doi: 10.1038/nature25480. Available online: https://pubmed.ncbi.nlm.nih.gov/29489754/ - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
