

AI-based CT Body Composition Identifies Myosteatosis as Key Mortality Predictor in Asymptomatic Adults
- PMID: 37191484
- PMCID: PMC10315523
- DOI: 10.1148/radiol.222008
AI-based CT Body Composition Identifies Myosteatosis as Key Mortality Predictor in Asymptomatic Adults
Abstract
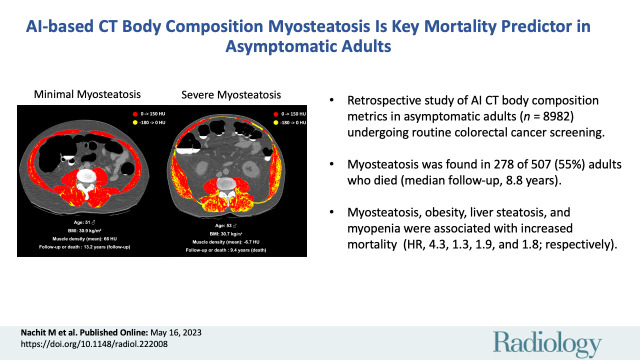
Background Body composition data have been limited to adults with disease or older age. The prognostic impact in otherwise asymptomatic adults is unclear. Purpose To use artificial intelligence-based body composition metrics from routine abdominal CT scans in asymptomatic adults to clarify the association between obesity, liver steatosis, myopenia, and myosteatosis and the risk of mortality. Materials and Methods In this retrospective single-center study, consecutive adult outpatients undergoing routine colorectal cancer screening from April 2004 to December 2016 were included. Using a U-Net algorithm, the following body composition metrics were extracted from low-dose, noncontrast, supine multidetector abdominal CT scans: total muscle area, muscle density, subcutaneous and visceral fat area, and volumetric liver density. Abnormal body composition was defined by the presence of liver steatosis, obesity, muscle fatty infiltration (myosteatosis), and/or low muscle mass (myopenia). The incidence of death and major adverse cardiovascular events were recorded during a median follow-up of 8.8 years. Multivariable analyses were performed accounting for age, sex, smoking status, myosteatosis, liver steatosis, myopenia, type 2 diabetes, obesity, visceral fat, and history of cardiovascular events. Results Overall, 8982 consecutive outpatients (mean age, 57 years ± 8 [SD]; 5008 female, 3974 male) were included. Abnormal body composition was found in 86% (434 of 507) of patients who died during follow-up. Myosteatosis was found in 278 of 507 patients (55%) who died (15.5% absolute risk at 10 years). Myosteatosis, obesity, liver steatosis, and myopenia were associated with increased mortality risk (hazard ratio [HR]: 4.33 [95% CI: 3.63, 5.16], 1.27 [95% CI: 1.06, 1.53], 1.86 [95% CI: 1.56, 2.21], and 1.75 [95% CI: 1.43, 2.14], respectively). In 8303 patients (excluding 679 patients without complete data), after multivariable adjustment, myosteatosis remained associated with increased mortality risk (HR, 1.89 [95% CI: 1.52, 2.35]; P < .001). Conclusion Artificial intelligence-based profiling of body composition from routine abdominal CT scans identified myosteatosis as a key predictor of mortality risk in asymptomatic adults. © RSNA, 2023 Supplemental material is available for this article. See also the editorial by Tong and Magudia in this issue.
Conflict of interest statement
Figures
![Flowchart shows patient inclusion and exclusion. Patients with missing
body composition data (body mass index [BMI], liver density, skeletal muscle
index [SMI], or muscle density) or with evident muscle artifacts at CT were
excluded before the univariable analysis. Multivariable analysis was
performed on the cohort with complete data available, including smoking
status, medical history of cardiovascular events, and visceral fat
measurements. (* = data were missing in 679 patients, when accounting
for overlaps.)](https://cdn.ncbi.nlm.nih.gov/pmc/blobs/fbf2/10315523/d64ac6d3299c/radiol.222008.fig1.jpg)



![Schematic shows possible transition states of the multistate Markov
model, starting at inclusion (ie, CT scan acquisition) and leading to
intermediate states (ie, major adverse cardiovascular events [MACEs],
indicated by gray circles) and/or to an absorbing state (ie, death or loss
to follow-up, indicated by red circles). Transitions numbered 2, 4, 6, 8, or
9 lead to an absorbing state and transitions numbered 1, 3, 5, or 7 lead to
an intermediate state. CV = cardiovascular.](https://cdn.ncbi.nlm.nih.gov/pmc/blobs/fbf2/10315523/46a4fe20ec3d/radiol.222008.fig5.jpg)

Comment in
-
One Step Forward in Opportunistic Screening for Body Composition.Radiology. 2023 Jun;307(5):e231003. doi: 10.1148/radiol.231003. Epub 2023 May 16. Radiology. 2023. PMID: 37191482 No abstract available.
References
-
- Blüher M . Obesity: global epidemiology and pathogenesis . Nat Rev Endocrinol 2019. ; 15 ( 5 ): 288 – 298 . - PubMed
-
- González-Muniesa P , Mártinez-González MA , Hu FB , et al. . Obesity . Nat Rev Dis Primers 2017. ; 3 ( 1 ): 17034 . - PubMed
-
- Prado CMM , Lieffers JR , McCargar LJ , et al. . Prevalence and clinical implications of sarcopenic obesity in patients with solid tumours of the respiratory and gastrointestinal tracts: a population-based study . Lancet Oncol 2008. ; 9 ( 7 ): 629 – 635 . - PubMed
-
- Martin L , Birdsell L , Macdonald N , et al. . Cancer cachexia in the age of obesity: skeletal muscle depletion is a powerful prognostic factor, independent of body mass index . J Clin Oncol 2013. ; 31 ( 12 ): 1539 – 1547 . - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
